Deniz Publication
Clinical Cancer Investigation Journal
ISSN Print: 2278-1668, Online: 2278-0513
ISSN Print: 2278-1668, Online: 2278-0513
Drug repurposing, exploring new uses for existing drugs, offers significant advantages over developing new ones. Repurposed drugs have already undergone safety testing, reducing failure chances. Pre-existing data and manufacturing knowledge shorten the process. Development is cheaper, with estimates at $300 million compared to $2-3 billion for new drugs. Repurposed drugs can reach the market in 3-12 years, versus 10-17 years for new drugs. Overall, drug repurposing is a promising approach for faster, cheaper development of new treatments. Colon cancer treatment faces hurdles. Traditional drug development is slow and expensive. This review highlights drug repurposing as a strategic solution. By finding new uses for existing drugs, we can overcome these challenges. This review explores various approaches for colon cancer drug repurposing: Network models: Identifying connections between drugs and diseases. Computer-aided approaches: Utilizing software to predict drug-target interactions. Machine learning algorithms: Analyzing vast datasets to uncover hidden patterns. Molecular docking techniques: Simulating how drugs bind to target molecules. This review highlights aspirin as a promising candidate for colon cancer repurposing. Its potential benefits aspirin may slow down cancer cell division. And also emphasizes the role of artificial intelligence and network modeling in drug repurposing. The drug repurposing presents a promising strategy for overcoming the challenges of colon cancer treatment. By leveraging cutting-edge computational approaches and personalized medicine, we can develop more effective and efficient treatment options for patients.
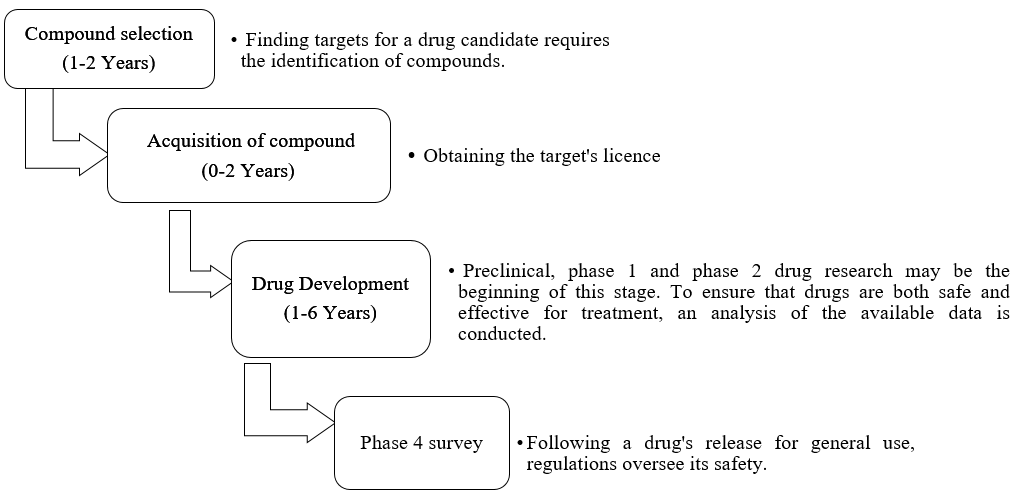
The exercise of drug repurposing, otherwise called therapeutic switching or repositioning, identifies fresh therapeutic applications for drugs already in existence, encompassing those that are old, unsuccessful, experimental, FDA-approved, or pro-drugs. This project goes beyond the original therapeutic role of these drugs to explore their hidden potential.[1] This method offers several benefits compared to creating a completely new drug for a specific medical purpose. As shown in Figure 1. First, since the repurposed medication has already been exhibited to be safe in preclinical tests and, if relevant, early human trials, there is a decreased chance of failure. In later efficacy trials, this lessens the likelihood of failure, particularly about safety concerns. Second, because a large number of preclinical trials, safety assessments, and occasionally development of formulation have already been finished, the overall development schedule may be shortened. Third, there's potential for reduced investment requirements, though this varies based on the repurposing candidate's development stage. Preclinical and phase I and II costs can be significantly reduced, even though phase III and regulatory costs might be comparable to those of new medicine in the same indication.[2] All these benefits add up to a lower average cost once failures are taken into account, reducing repurposed drug development risk and returning on investment faster. It is estimated that the average price to bring a repurposed drug to market is $300 million, while the price of a new chemical entity is estimated to be between $2 and $3 billion. Furthermore, repurposed medications might identify fresh targets and lines of inquiry.[2] Research indicates that the duration required to develop and identify novel medications may range from 10 to 17 years. Repurposed drugs, however, are usually approved at a cost of approximately half that of original medications and within a time frame of three to twelve years.[3]
|
|
|
Figure 1. There are four stages of Drug repurposing 1) Compound selection, 2) Acquisition of compound, 3) Drug development, 4) Phase 4 survey |
Cancer is still a serious medical problem with many unmet needs, even with recent years seeing tremendous advancements in cancer treatment options. As such, to tackle this intricate illness, scientists are working nonstop to develop new treatment approaches.[4] Finding new uses for already-approved medications is called drug repurposing, and it has become a potentially effective treatment option for cancer. Researchers from academia and industry are paying more and more attention to this tactic, which presents a viable means of accelerating the development of cancer treatments.[5]
In the United States of America, colon cancer ranks as the second leading cause of cancer-related deaths. The American Cancer Society meticulously compiles and updates CRC statistics every three years, drawing upon incidence data from population-based cancer registries and mortality data from the National Centre for Health Statistics. For the year 2023, projections indicate that approximately 153,020 individuals will receive a CRC diagnosis, and 52,550 will succumb to the disease. Notably, among these cases, 19,550 diagnoses and 3,750 deaths will occur in individuals younger than 50 years old.[6]
As first lines of defence against the disease, surgery, and chemotherapy have been used for many years to treat cancer patients. Some other available treatments are gene therapy, immunotherapy, adoptive T-cell therapy, complement inhibition, cytokine therapy, and natural product therapy.[7]
Although the monitoring of colorectal metastases has not changed much over the past ten years, advancements in liver-directed and systemic therapies may improve survival rates. Instead, a new era of image- and pathology-guided therapy has been ushered in by creative approaches to the treatment of rectal cancer.[8] Promising data supports comparable long-term outcomes with non-surgical methods; anticipated changes in rectal cancer treatment include identifying complete responders before surgery. Except for patients who experience a local recurrence following neo adjuvant therapy, this implies a possible shift away from radical surgery for some patients. Precise therapy response monitoring techniques are essential to navigating these developments and improving patient care for patients with stage IV colon cancer.[8]
Repurposing drugs has enormous promise to help patients with rare, orphan, and neglected diseases find unmet medical needs. This approach can speed up the development of new therapies and enhance patient outcomes by making use of the knowledge and resources that already exist.[9] Drug repurposing already-approved pharmaceuticals has the potential to overcome the shortcomings of the current drug pipeline for specific diseases, resulting in more accessible treatment choices, substitute drugs, and therapies with more tolerable side effects.[10] The difficulties in finding new drugs include rising research and development (R&D) expenses, a protracted drug development process, a poor success rate, and regulatory obstacles.[11] The pharmaceutical sector also faces competition from generics and off-label prescriptions, as well as revenue loss due to patent expiration. From an industrial standpoint, drug repurposing is said to be less expensive, time-consuming, risky, and to have a higher likelihood of success.[12]
Numerous databases and computational tools, including Drug Predict, Drug Bank, Promiscuous, Mantra2.0, Pharm DB, DRAR-CPI, repoDB, Repurpose DB, DeSigN, Cmap, and DPDR-CPI, can be used for drug repurposing.[13] Computational techniques like data mining, machine learning, &analysis of networks are required due to the growing availability of large-scale biomedical data to yield more trustworthy results. These techniques are key to the systematic repositioning of drugs, identification of therapeutic potentials, and discovery of new uses for already-approved medications, particularly in the treatment of difficult diseases like cancer.[14]
Using a variety of data sources, machine learning-based models can look into repositioning opportunities and, by checking underlying systems, forecast new drug-disease associations. In the past few years, there has been an increasing number of proposed methods of machine learning, especially when mixed with the elucidation of different features, enhancing their effectiveness.[15] Machine-learning models developed by Menden et al. [16] predict how cancer cell lines will react to medication therapy based on IC50 values. To develop feed-forward perceptron neural network model and a random forest regression model, the model combined chemical properties (like structural fingerprints) and cancer genomic features (like the status of seventy-seven oncogene mutations and micro-satellite status). The predicted IC50 values were then subjected to cross-validation as well as a non-dependent blind test to confirm their accuracy. Napolitano et al. [17] concentrated on a drug-centric strategy for anticipating the therapeutic class of drugs. They employed drug-related features, such as similarity in chemical structure, molecular target, and gene expression, to form a consolidated drug similarity matrix. This matrix served as a kernel for SVM classification. In addition to features related to drugs, Gottlieb et al.[18] incorporated diverse disorder-related features, including not only genetic but also phenotypic characteristics. Using these features, they calculated measures of similarity between drugs and between diseases to create classification features. Subsequently, they applied a logistic regression classifier to forecast new drug applications. In addition, there are machine learning algorithms that predict unknown relationships between medications and illnesses by using collaborative filtering techniques. Zhang et al.[19] provided a thorough computational framework, for instance, that integrates different aspects of disease and drug similarity. Essentially, to create drug similarity and disease similarity matrices, phenomics variables (disease phenotype and drug side effects), genomic features (drug target protein and disease gene), and chemical structure information (drug chemical structure) were combined. The authors turned the drug-disease network analysis into an optimization problem by employing this collective data. The computational framework exhibits noteworthy efficacy in identifying novel prospective therapeutic indications. Yang et al.[20] inferred relationships between medications and illnesses using a causal inference-probabilistic matrix factorization technique. This model establishes causal networks between disease, gene, target, pathway, and drug by integrating multiple levels of relations. Based on well-known interactions, PMF modes were discovered. With the ability to forecast new drug-disease correlations, this method provides insightful information for drug repositioning.
The models show nodes to showcase things like drugs, diseases, or gene products, and edges to present the relationships or associations among them. Based on knowledge or computational inferences made using a range of data sources, these networks illustrate different types of interactions, such as drug-drug, drug-target, drug-disease, disease-disease, disease-gene, and protein-protein interactions, as well as transcriptional and signal networks.[21] This method can uncover previously undiscovered or concealed relationships among drugs and diseases by merging different data sources and applying the 'guilt-by-association' principle. This hypothesis suggests that drugs with comparable transcriptional responses might also function similarly.[22] The comparison of target-based, drug-based, and network-based interactions with a bi-partite network to assess their similarities. They found that, when evaluated by the area under the receiver operating curve (AUROC), network-based inference performed the best when they used these commonalities to forecast drug-target interactions.[23] Furthermore, employed a heterogeneous network model for drug-disease interactions, wherein they pinpointed closely interconnected modules of drugs and diseases.[24] This method made it easier to extract data from drug-disease pairs about possible candidates for medication repositioning. Using potential off-target effects on cancerous cell signaling pathways, they proposed a method for repurposing cancer medications.[25]
We discovered a meta-signature of genes at this point in the investigation that can identify colon cancer tissues from healthy tissues with accuracy.[26] A noteworthy feature that also surfaced was the significance of variables in various models. The most important variables from the 3 methods (Random Forest, Glmnet, and edgeR) appeared to significantly overlap, suggesting that these genes may play an important role in the illness. In light of this, we think it is essential to carry out an in-silico investigation to track the connections between these genes' protein products and various FDA-approved anti-cancer drugs.[27] Some examples of repurposed drugs as shown in Table 1.
|
Table 1. Some examples of repurposed drugs. |
|||
|
Name of drug |
Initial indication |
Repurposed indication |
Approach used for repurposing |
|
Minoxidil |
Hypertension |
Hair loss |
Clinical analysis conducted retrospectively |
|
Sildenafil |
Angina |
Erectile dysfunction |
Retrospective clinical analysis |
|
Atomoxetine |
Parkinsonism |
Attention-deficit hyperactivity disorder |
Pharmacological analysis |
|
Raloxifene |
Osteoporosis |
Cancer of breast |
Retrospective clinical analysis |
|
Duloxetine |
Analgesia |
Premature ejaculation |
Pharmacological analysis |
|
Topiramate |
Epilepsy |
Obesity |
Pharmacological analysis |
|
Ketoconazole |
Fungal infection |
Cushing syndrome |
Pharmacological analysis |
|
Rituximab |
Various cancer |
Rheumatoid arthritis |
Historical analysis: rheumatoid arthritis remission in patients receiving rituximab for non-Hodgkin lymphoma. |
|
Zidovudine |
Cancer |
HIV or AIDS |
Screening compound libraries in a controlled laboratory setting. |
|
Thalidomide |
Morning sickness |
Multiple myeloma |
Non-approved application % pharmacological examination. |
|
Aspirin |
Analgesia |
Colon cancer |
Retrospective analysis of pharmacological and clinical data. |
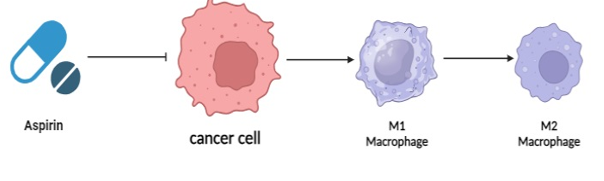
Acetylsalicylic acid i.e. Aspirin represents the earliest illustration of drug repurposing. Since 1968, extensive research has been conducted on the qualities that prevent cancer of aspirin, a medication mostly used for pain relief. Both COX-dependent and independent pathways are involved in the aspirin's mode of action.[28] Its anti-tumor efficaciousness against various tumor types has also been reinforced by pre-clinical research.[29] Aspirin has been studied for its possible effects against cancer as a non-steroidal anti-inflammatory drug (NSAID).[30] Though the precise mechanisms are unknown, it is believed that inhibition of cyclooxygenase (COX) activity plays a role, especially in colorectal cancer.[31] As shown in Figure 2. aspirin suppresses immune response by preventing M1 macrophages from polarizing and changing into M2 macrophages.[32] The potential synergistic anticancer effects of aspirin and anti-PD-L1 blockade together to inhibit COX in human tumours have been studied.[33] Clinical studies have shown the efficacy of aspirin in preventing colon cancer.[34]
|
|
|
Figure 2. Aspirin prevents the conversion of cancer-promoting macrophages (M1 and M2) by blocking COX activity, which enhances the anticancer immune response.[35] |
There have been significant efforts over the last few decades to find new ways to treat cancer. Even so, still, cancer is one of the leading causes of death worldwide. In the process of developing new drugs, accepted known molecular entities that are applied in non-cancerous contexts are explored in addition to de novo design.[36] Colon cancer ranks second globally in terms of cancer-related mortality. The main causes of colon cancer are discovered to be mutations in the TP53 gene.[37] TP53 is the gene that codes for the p53 protein.[38] Through apoptosis or autophagy, p53 can permanently eliminate irreparably damaged cells in addition to encouraging the survival and repair of damaged cells.[39] Thus, tumor incidence and progression can be prevented by the intricate regulation of p53.[39] The discovery that non-oncology drugs have anticancer activity has been made possible by advances in genomics and drug screening.[40]
The field of finding CRC biomarkers has advanced significantly. This is made feasible by advancements in biomarker identification techniques including organoids, patient-derived xenografts, liquid biopsies, and CMS characterization. To create the gold standard for biomarker development, more prospective validation is therefore required. To ensure that this standard is clinically viable, more study is needed, namely addressing challenges of quantification, repeatability, and commercial scalability.[41] Mechanism-based medicines, which are focused on the tumor's molecular profile rather than its anatomical location or type of tissue, are replacing typical staging-based therapies for the treatment of patients with advanced colon cancer. Thanks to the updated CRC categorization, treatment can now be customized based ona CMS subtype.[42] Currently, the approaches used to describe CMS are challenging to utilize in clinical settings, particularly when attempting to extract high-quality genome-wide transcriptome data from paraffin-embedded, formalin-fixed tissue. But recent research has shown that CMS-based classifiers based on immunohistochemistry (IHC) can reach 87% concordance with the gold standard transcriptome-based classification using five markers (CDX2, FRMD6, HTR2B, ZEB1, and KER).[43] In the field of biomarker discovery, patient-derived xenografts are becoming more and more important. Tumor cells from a patient are transplanted into immunodeficient mice in this experimental cancer model.[44] Patient-derived tumor organoids are another cutting-edge tool for the discovery of biomarkers. These three-dimensional in vitro models have a great deal of potential for application as an ex-vivo platform to predict and customize treatment results for patients.[45] Moreover, there is a great deal of promise for improving combinatorial drug therapies and repurposing drugs with unidentified therapeutic benefits. Organoid technology allows for high-throughput filtering, which makes this possible.[46]
Through advances in deep learning, artificial intelligence (AI) provides computer-aided solutions that benefit patients with colorectal cancer (CRC). Lesion detection and diagnosis are aided by these techniques, which result in individualized treatment plans. While computer-assisted systems remove observer variability and distractions, technology increases the speed and accuracy of diagnosis. When it comes to CRC diagnosis and detection, AI tools can currently either equal or even surpass human performance.[47] AI systems are also employed in the evaluation of screening and diagnostic procedure quality. Indeed, researchers created and evaluated a model to gauge colonoscopy quality across several institutions using natural language processing (NLP).[48] A multitude of AI-enabled virtual assistants offer personalized healthcare services and enhance communication among patients and providers as well. Furthermore, community education can be enhanced and CRC screening program participation increased with the help of mobile AI apps like Colour App (Colorectal Cancer Awareness Application).[49] Although AI applications offer substantial benefits for both CRC diagnosis and treatment, there are several obstacles facing the advancement of AI-based technology. It is a challenging task that relies on numerous factors to educate a machine to think like a person. One significant barrier to the advancement of AI is the integration and widespread application of this cutting-edge technology in clinical workflows. It is anticipated that the use of AI tools in routine patient care will increase as new approvals from regulatory bodies and professional associations surface. Creating AI models is acknowledged as a notably costly process, in addition to difficulties with FDA approval.[50] There are further privacy-related issues with this cutting-edge technology. The possibility of deliberate privacy breaches may rise in the event of collaborations between academic research data and healthcare companies. These systems can be equipped with artificial intelligence (AI)-based platforms that can evaluate data from an electronic medical record (EMR) or a colonoscopy film. This way, the information can be used for training or real-time decision assistance. Deep learning techniques have been used by medical professionals and researchers in recent years to analyze large databases and find hidden opportunities within them. AI tools help physicians assess a patient's medical history and choose the best course of action. Because of this, this cutting-edge technology has a lot of potential for handling and processing large datasets. To create appropriate security and privacy protocols for the secure storage and handling of medical data, more research is needed.[50]
Finding new treatments for colon cancer can be revolutionized by investigating medication repurposing tactics, especially with the use of computational approaches like machine learning, network modeling, and docking studies. These computational tools speed up drug discovery by methodically studying already-approved medications, offering an affordable substitute for more time-consuming techniques. Given its well-established safety profile and well-documented anti-cancer capabilities, the exemplary case of aspirin highlights the potential effectiveness of repurposing. The challenges of pharmacological repurposing, despite their potential, must be carefully considered. Obstacles such as off-target impacts and restricted patent protection need more sophisticated approaches and laws. Recognizing these obstacles is essential to reducing risks and guaranteeing that repurposed medications are successfully converted into colon cancer therapies. To further medication repurposing, it appears that integrating biomarkers with artificial intelligence is essential. The utilization of biomarkers facilitates accurate patient categorization, hence augmenting the probability of favourable therapy results. In the meantime, by finding promising candidates and projecting their efficacy, artificial intelligence, with its data-driven predictive modeling skills, holds the potential to completely transform the drug discovery process. All things considered, this talk emphasizes the possibility of medication repurposing in colon cancer, utilizing computational techniques and providing aspirin as an example of successful use. A more effective and individualized approach to colon cancer therapies is made possible by addressing obstacles and integrating cutting-edge technology like biomarkers and artificial intelligence. This strategy promises better patient results and moves the field closer to precision medicine.
The investigation of medication repurposing in colon cancer, especially with aspirin, indicates a viable path for resolving treatment-related obstacles, to sum up. Aspirin has emerged as a notable possibility for the identification and validation of repurposed pharmaceuticals, thanks to the extensive integration of computational tools, machine learning, and molecular docking approaches. According to our predictions, developments in customized medicine and artificial intelligence will be crucial in enabling us to customize treatments for each patient. This review highlights the possibility of a paradigm change in colon cancer treatments with its thorough understanding of repurposing tactics. The review endeavours to direct researchers and clinicians towards more efficacious and focused interventions by tackling obstacles and highlighting customized methods. The numerous ways that aspirin is being used in medication repurposing provide a glimmer of hope for better colon cancer treatment outcomes as the field develops, opening the door for a sophisticated, patient-cantered, and innovative approach to cancer therapy.
The authors would like to thank the Management and Principal of DPU Pharmacy for providing the necessary support and facilities to write this review.
None.
None.
None.
|
||||||||