Deniz Publication
Clinical Cancer Investigation Journal
ISSN Print: 2278-1668, Online: 2278-0513
ISSN Print: 2278-1668, Online: 2278-0513
Hyperthermia (also called heat therapy or thermotherapy) is a cancer treatment method in which body tissue is exposed to high heat (up to about 113 degrees Fahrenheit). Hyperthermia shrinks tumors by destroying cancer cells and damaging the proteins and structures inside the cells. The purpose of this research is to introduce the hyperthermia treatment technique as an additional treatment method. This technique is applied topically, deep, hyperthermia, and intra-tumor in the whole body. Based on the results obtained from various studies, hyperthermia together with chemotherapy or radiation therapy or both methods, without significantly increasing side effects, increases the tumor response to treatment, local control of the tumor, pain relief effects, and the survival rate of patients. Many advances that have been made in recent years in the field of physical thermometry, hyperthermia, and modeling techniques in treatment design have increased the use of this treatment method in different countries. Today, in the treatment of breast, glioblastoma, melanoma, cervical, bladder, rectal, and cervical tumors, it is recommended to add hyperthermia to the usual treatment regimens. Since this technique is not well introduced in some countries, the need to fully understand it is obvious.
Today, to eliminate cancerous tumors and improve the treatment outcome, much attention has been paid to combined treatment regimens.[1-3] Undoubtedly, the reason for using other treatment regimens along with radiation therapy is to prevent tumor recurrence.
One of the most important reasons for tumor recurrence is the presence of hypoxic cells in the central area of tumors. These cells have a lower pH than the peripheral cells of the tumor. These conditions make the cells in the central area of the tumor more resistant to x and γ rays. Since the oxygen enhancement ratio (OER: oxygen enhancement ratio) for these rays is about 2-3, to cause a certain amount of damage in hypoxic conditions, the radiation dose must be increased 2-3 times, which is the dose received by healthy tissues.[4] Many efforts have been made to overcome this problem, the most important of which are: using oxygen with a pressure of 2-3 atmospheres during radiation therapy; the use of sensitizing drugs that specifically affect hypoxic cells; using rays with high linear energy transfer (LET: linear energy transfer), using hyperthermia technique.[4-6]
This article introduces the hyperthermia treatment method, which is used as an additional treatment method along with radiation therapy and chemotherapy. Of course, many treatment methods such as gene therapy, stem cell transplantation, immunotherapy, etc. It has been used in Western countries for several decades, but it has been neglected in some countries.
The purpose of this article is to provide an overview of this method and introduce it, and most of the discussions are focused on the technique of this topic.
Hyperthermia is derived from the Greek words hyper meaning high and therme meaning heat, meaning a controlled increase in temperature from 37 to 45-40 degrees Celsius to treat tumors. Since 5000 BC, it has been recognized that taking a warm water bath and increasing the body temperature is an effective method for treating infectious and malignant diseases.[7] Years ago, scientists discovered that cancer cells are more sensitive to heat than
Studies show that applying temperatures higher than 45 degrees directly causes cell death due to coagulation of proteins. Inducing such heat in deep tumors of the human body is not an easy task; Therefore, most of the results that can be seen from the effect of hyperthermia in the treatment of tumors are not directly caused by an increase in cell death, but by an increase in blood flow in the vascular system of the tumor and as a result, an increase in the oxygen pressure of the cell, an increase in the pH of the cell, destruction of the skeleton, and the membrane cell and finally the disruption of the physiological functions of the cell nucleus, all of these factors cause irreparable damage and finally cell death.[8-10] On the other hand, the increase in temperature by affecting the function of cell proteins prevents the process of DNA damage repair, it causes the damage to stabilize in the cell, which increases cell death.[11] In addition, cells in the S phase of the cell cycle show more relative resistance to radiation therapy but are more sensitive to heat. An increase in temperature also increases the rate of absorption and effect of chemotherapy drugs. In general, there is no difference between healthy and cancerous cells in terms of heat sensitivity, except for malignancies in blood cells, but since the substrate, the vascularity of most tumors (solid tumors) is irregular, in which hypoxic cells with low pH are seen more often.[12-14] In this situation, cancer cells show relative resistance to radiation, while they are more sensitive to heat.[15] Therefore, hyperthermia acts as one of the most important radiation and chemical sensitizers.
The above content justifies the use of a combined treatment regimen of radiation therapy with hyperthermia, which is usually prescribed for a maximum of six sessions (one session per week) during radiation therapy. Radiation therapy destroys oxygenated cells around the tumor, and hyperthermia affects the central hypoxic cells of tumors, making them more sensitive to radiation. In this context, two factors should be considered.
The first factor is the Thermal Enhancement Ratio. At a temperature of about 40-45 degrees, this ratio is about 2-1.5, that is, to cause a certain number of damage in the cells in the absence of hyperthermia, the radiation dose should be increased by 1.5-2 times. In addition, the value of TER is higher in hypoxic conditions and increases with increasing temperature, increasing the duration of heat application and decreasing the time interval between radiation therapy and hyperthermia. Maximum TER is achieved when hyperthermia is applied simultaneously with radiation therapy. Studies have shown that in this case, the benefit of treatment increases by 1.5-2 times.[16-18] Of course, the simultaneous application of hyperthermia and radiation therapy for all patients and all tumors is technically not possible; therefore, hyperthermia should be applied before or after radiation therapy. Many studies have been conducted in this field, and most of them have concluded that applying hyperthermia up to six hours after radiation therapy has a beneficial effect on increasing the therapeutic benefit.[17-21]
The second factor is Thermotolerance. By applying a temperature of 43 degrees and above for 40-60 minutes, many tumoral cells are destroyed, but in the meantime, some cells survive. The remaining cells acquire a relative resistance to heat, which is called thermotolerance. The higher the initial temperature, the higher the induced thermal resistance.[22, 23]
In the hypoxic areas of tumors due to insufficient blood flow, the concentration of drugs used in chemotherapy is low, but many of these drugs can increase their anticancer effect with increasing temperature. Studies show that for many drugs, adding hyperthermia can increase the sensitivity of tumor cells to these drugs. An accepted mechanism in this field is that with the increase in temperature, the blood flow in the tissue increases and increases the absorption of drugs. After that, the concentration of the drug inside the tumor is increased as a result of DNA damage and its cell-killing effects also increase.[24, 25]
The intensifying effect of hyperthermia is observed when it is applied at a time close to chemotherapy, that is when there is a suitable concentration of the drug in the tumor area. This intensification depends on the amount of temperature and the duration of heat application and has been reported for 1.2-10 different drugs. Of course, in some studies, no appreciable aggravation effect has been seen.[26]
Today, the application of the combined treatment regimen of radiation therapy, chemotherapy, and hyperthermia has received significant attention. For the first time in 1988, Japanese scientists used this treatment regimen clinically (to treat esophageal cancer) and obtained very good results. Recently, other studies have been conducted in the treatment of head, neck, breast, and rectal tumors, which have brought valuable results.[27, 28] Westermann et al.[29] published the positive results of an extensive study in which patients with cervical cancer were treated using these three methods in medical centers in the Netherlands, Norway, and the United States.
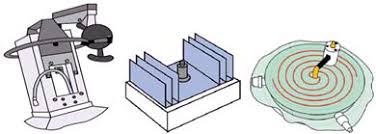
In this technique, microwave (MW) antennas, ultrasonic wave generator applicators, and radio wave (RF) generator applicators are used. Today, in most hyperthermia centers, RF wave generator applicators are used, the most important of which are shown in Figure 1, and their commercial types are available with a diameter of about 15 cm and a frequency of 50-340 MHz. These applicators are suitable for tumors up to a depth of about 3 cm.[30] In all hyperthermia techniques, an intermediary substance (usually water) is placed between the applicator and the skin, which causes better contact between the applicator and the skin and prevents side effects on the skin.
|
|
|
Figure 1. Some examples of applicators used in local surface hyperthermia. |
These two techniques are suitable for treating tumors with a maximum diameter of 5 cm. In intratumoral hyperthermia, a heat-generating source is installed inside the tumor. In the intracavitary hyperthermia method, the related antenna or electrode is placed in contact with the tumor through the opening of the natural cavities of the body.[30] In these methods, to achieve uniform heat distribution, the distance between the electrodes should not be more than 1.5 cm, so more electrodes are needed, which makes this technique considered very invasive.[30] On the other hand, in this method, the interference of the waves radiated from multiple electrodes together causes more non-uniformity of the energy in the treated area, and therefore uniform heat will not reach the tumor. Research in this field continues to achieve a more uniform distribution of heat in the tumor.
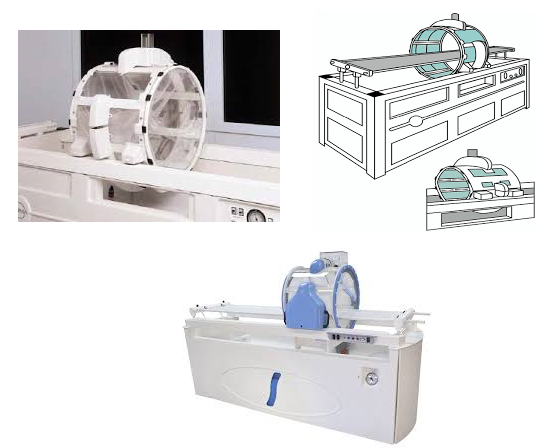
For hyperthermia of deep tumors, special applicators are used in which the patient or the related organ is placed, and RF waves are sent to the treated area after being radiated from the antennas around the applicator and passing through a layer of water (Figure 2). The most famous of them are Sigma applicators, which have at least 4 pairs of RF-generating antennas and are designed in the form of a cylinder with a cross-sectional diameter of 30-40 and 60 cm. The 30-Sigma applicator (with a diameter of 30 cm) is used for hyperthermia of lower limb tumors. For abdominal and pelvic tumors, the 40-sigma applicator (with a diameter of 40 cm) is used in children and the 60-sigma applicator (with a diameter of 60 cm) is used in adults.[31] The 60-Sigma applicator, which produces waves with a frequency of 70-120 MHz, is one of the most widely used applicators in the treatment of deep tumors, which is used in most hyperthermia centers around the world.
|
|
|
Figure 2. Different applicators are used in deep hyperthermia. |
Of course, this system has two disadvantages, firstly, the control of energy distribution in this applicator is limited. Energy control and regulation in a three-dimensional volume can only be implemented in one direction. To solve this problem, another applicator has been designed that has 12 pairs of antennas and produces waves with a frequency of 100 MHz. The cross-section of this applicator is in the shape of an eye and that is why it is known as Sigma-Eye. Its dimensions are 58 x 38 cm. Of course, the latter applicator cannot be used for large-sized patients due to its special type of design. The second disadvantage of the 60-Sigma applicator is that due to its relatively large diameter, the thickness of the water layer around the patient is also relatively large, which causes a lot of pressure to be applied to the patient's stomach and internal organs during the hyperthermia application. To solve this problem, a new applicator called Sigma-60-Ellipse has been designed, the size of its oval opening is 38 x 58 cm. Preliminary studies show that this applicator is a suitable alternative to previous applicators.[32]
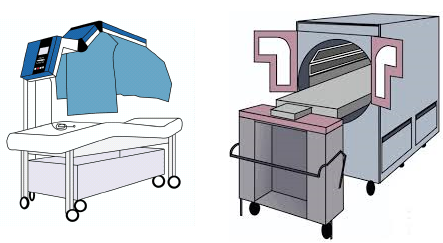
This technique is used to treat patients who suffer from metastases throughout the body. The physical technique that is used in the clinic today is the use of systems that transfer heat in the form of radiation. One of the most famous whole-body hyperthermia systems is the Aquatherm cabin, which is a chamber saturated with moisture, hot water pipes (with a temperature of 50-60°C) are installed inside and the patient is placed inside. These tubes act as radiators emitting infrared (IR) waves.[30] Iratherm is another system used for whole-body hyperthermia. In this system where the patient is placed, IR radiators are the source of heat energy radiation to the body (Figure 3).
|
|
|
Figure 3. Devices used in whole-body hyperthermia. |
Measuring, recording, and analyzing information related to temperature and its distribution in the tumor and adjacent tissues, which is done to check and control the quality of treatment, is one of the necessities of hyperthermia. For this purpose, thermocouples, thermistors, or optical fiber thermometers are used. After recording and sending the data, various thermal indices are calculated and three-dimensional curves (temperature-time-length) are drawn. Therefore, at any time, at any depth of the tumor, its temperature is available.[33-35]
In hyperthermia, dosimetry is usually done in the following ways: For surface tumors, thermometers are installed on the surface of the skin. There are two different views about deep tumors. Some people believe that thermometry should be done interstitially.[36] In the second point of view, experts believe that if the tumor is located in an area that is accessible through the natural lumens of the body, thermometry should be performed intraluminally.[37, 38] Since intratumor thermometry is very painful, time-consuming, and expensive for the patient, and in some cases causes infection and even tumor seeding in the counter, on the other hand, it does not provide more information for energy control and heat distribution. Today, in most centers, thermometry is performed intraluminally.
The Magnetic Resonance Thermometry method has recently been used in two hyperthermia centers in Durham (USA) and Berlin (Germany) and is a non-invasive method.[39] In this method, the patient enters the MRI gantry while he is placed inside the hyperthermia applicator, and the information related to the temperature distribution in all points of the tumor is imaged and recorded by the MRI system. Although this method is expensive, its very high resolution shows the temperature distribution in a valuable way.[40]
Results and Discussion
The effect of hyperthermia in the treatment of tumors has been shown in various clinical studies. Falk and Issels reported the results of 17 phase 1 and 2 studies under the title "The art of hyperthermia", in all of which the effect of combining hyperthermia with radiation therapy and chemotherapy showed a significant difference with similar treatments (without hyperthermia).[41]
Van der Zee, in a comprehensive article, presented the results of 27 phase 3 studies conducted around the world until then, and in 19 studies using hyperthermia with radiation therapy, and chemotherapy, both showed significant differences with similar treatments (without hyperthermic actions) showed.[42] In most studies,[42-44] the results show that there is a significant difference between radiation therapy alone and radiation therapy combined with hyperthermia; In addition, no significant side effects have been reported in any of the studies. In hyperthermia, due to non-uniform heat distribution and thermometric limitations, it is not possible to prevent the increase in temperature in the surrounding healthy tissues. On the other hand, the patient cannot always feel hot spots (such as those that have been operated on in the same area).
The side effects of the product in superficial hyperthermia are first and second-degree burns of the skin, which are seen in 25% of patients and are easily treatable.[45, 46] In deep hyperthermia, the skin is cooled extensively by water flow (inside the bag between the radiation source and the body); therefore, very hot spots appear in deep tissues under the skin. An increase in the temperature of fat under the skin or muscle tissue somehow causes pressure, which, of course, is not always detectable by the patient. The burning of subcutaneous fat and muscle tissue (which has been seen in 3-12% of patients) does not cause pain and discomfort, but the patient only feels the formation of a lump under his skin, which is fleeting and lasts at most for one or two weeks. It disappears by itself.[46-48] The important point is that studies in which hyperthermia and radiation treatment regimens have been used have not reported significant side effects.
In a study published by the Rotterdam Hyperthermia Group, peak nerve toxicity was observed in less than 1% of patients with tumors in the pelvic region, which, of course, did not prevent hyperthermia.[49] Whether or not side effects are exacerbated following hyperthermia in a regimen combined with chemotherapy depends on the temperature-induced in the treated tissue. The observed side effects have been described as acceptable according to the clinical results that this treatment regimen provides.[50]
Applying hyperthermia as an additional treatment method along with radiation therapy, chemotherapy or both can be done technically. Phase 3 studies have reported very valuable results in tumor treatment, local tumor control, and increasing the survival rate of patients up to twofold.
Laboratory and experimental studies have shown that hyperthermia increases the sensitivity of tumors to radiation therapy and chemotherapy. While the peripheral parts of the tumor are more sensitive to radiation, its central hypoxic cells show more relative resistance to radiation. It has been proven that central hypoxic cells of tumors become more sensitive to radiation under the influence of relative hyperthermia. This fact justifies the use of combined radiation therapy and hyperthermia; Radiation destroys tumor peripheral cells, and hyperthermia increases the effect of radiation in the central cells of the tumor. In addition, increased tumor blood flow (under the influence of hyperthermia) increases the effect of chemotherapy drugs. This issue also justifies the use of chemotherapy and hyperthermia compound treatment methods. On the other hand, studies have shown that hyperthermia not only does not increase the side effects of other treatment methods, but the side effects it causes are very limited and acceptable. Therefore, nowadays, in the treatment of various tumors, adding hyperthermia to the usual treatment regimens is recommended, and many patients benefit from these combined treatment methods.
Conclusion
Despite the remarkable therapeutic results that have been reported from hyperthermia as an adjunctive treatment method. Unfortunately, for the following reasons, this method of treatment is not yet fully known around the world. The first reason is that the results of the first randomized trial conducted in the United States did not show a successful therapeutic effect, which is explained by the inappropriateness of the therapeutic techniques. The report of this study hurt the view of scientists who did not show much interest in using this treatment method. Fortunately, the positive results of subsequent extensive studies completely changed this view.[51] For the second reason, most of the early studies showing the positive clinical effect of hyperthermia were conducted in Russia and Asia and received less attention than the failed American study. These cases caused the community of oncologists not to act with certainty regarding the use of hyperthermia.[26] Another effective issue in the general lack of recognition of hyperthermia is the issue of advertising. Studies have shown that hyperthermia alone increases the complete tumor response to treatment by 13% while adding it to radiation therapy can increase the rate of response to treatment by twofold.[42]
Today, in the treatment of breast, glioblastoma, melanoma, cervical, bladder, rectal, and cervical tumors, it is recommended to add hyperthermia to the usual treatment regimens. Since this technique is not well introduced in some countries, the need to fully understand it is obvious.
None.
None.
None.
None.
|
||||||||