Deniz Publication
Clinical Cancer Investigation Journal
ISSN Print: 2278-1668, Online: 2278-0513
ISSN Print: 2278-1668, Online: 2278-0513
Urinary Bladder Primary Squamous Cell Carcinoma: A Rare Case Description and Literature Review
Banyameen Iqbal1*, Harsh Kumar1, Vidya Vishwanathan1, Meesha Zaheer1, Charusheela Gore1
1Department of Pathology Dr. D.Y Patil Medical College, Hospital and Research Centre, Dr. D.Y Patil Vidyapeeth, Pimpri, Pune – 411018, India.
Abstract
Cancer of the urinary bladder is a commonly encountered malignancy of the urinary tract. The most common histologic type is Transitional cell carcinoma (TCC). It accounts for 90-95% of all bladder cancers. It is usually seen in the sixth and seventh decades of life. Men are affected three to four times more than women. The remaining 5-10% of the bladder tumors are other types of epithelial and mesenchymal tumors. Squamous cell carcinoma (SCC) of the urinary bladder is a very uncommon malignancy. It accounts for only 1-3% of all bladder cancers. Bladder tumors with only focal squamous differentiation are not diagnosed as SCC. Unfortunately, SCC of the urinary bladder is usually diagnosed at a late stage, and consequently, the prognosis is poor. The only proven predisposing factor implicated in the causation of SCC bladder is chronic irritation as by chronic urinary tract infections, bladder stones, schistosomiasis, etc. We present a case of SCC of the urinary bladder in a 70-year-old male patient who presented with hematuria, pain, and decreased frequency of micturition. A transurethral biopsy was performed at the site of the thickening of the bladder wall. The histopathological examination of the sampled tissue confirmed the diagnosis of a well-differentiated SCC.
Keywords: Bladder neoplasm, Malignant tumor bladder, Squamous cell carcinoma, Urinary bladder
Malignant tumors of the urinary bladder are commonly encountered in clinical practice.[1-4] It usually affects the elderly population and males are affected three to four times more than females. Most bladder cancers (90–95%) are urothelial carcinomas. Other epithelial and mesenchymal tumors are to blame for the remaining 5–10% of cases.[1, 5, 6] Squamous cell carcinoma (SCC) is extremely rare. Only 1-3% of all bladder malignancies are caused by it.[7] It is of interest to note that the incidence of bladder cancer differs significantly from country to country. This has been attributed to various social, environmental, occupational, and dietary carcinogenic factors. Common among these factors are chemicals, dyes, rubber, paint, textile, and leather work. Prolonged irritation of the bladder mucosa by calculi, infections, and schistosomiasis have also been implicated.[1, 6] In the majority of cases, a bladder tumor is a conventional urothelial or transitional cell carcinoma (TCC). However, sometimes foci of divergent differentiation with other histological types of malignancies like SCC, adenocarcinoma, micropapillary carcinoma, and neuroendocrine tumors may be observed. In such a situation, the tumor continues to be classified as urothelial carcinoma. A diagnosis of adenocarcinoma, SCC of the urinary bladder is reserved only for those tumors which exhibit essentially a pure histopathological tumor pattern.[1, 8]
70-year-old male patient came to the department of Urology with the complaint of painless hematuria of 15 days duration. He gave a history of recurrent urinary tract infections and off late was also having decreased frequency of urine. The patient was a chronic smoker and hypertensive for which he was on treatment. No other significant past, occupational or family history was given. The hematological parameters of the patient were within normal range. A urine examination showed the presence of red blood cells.
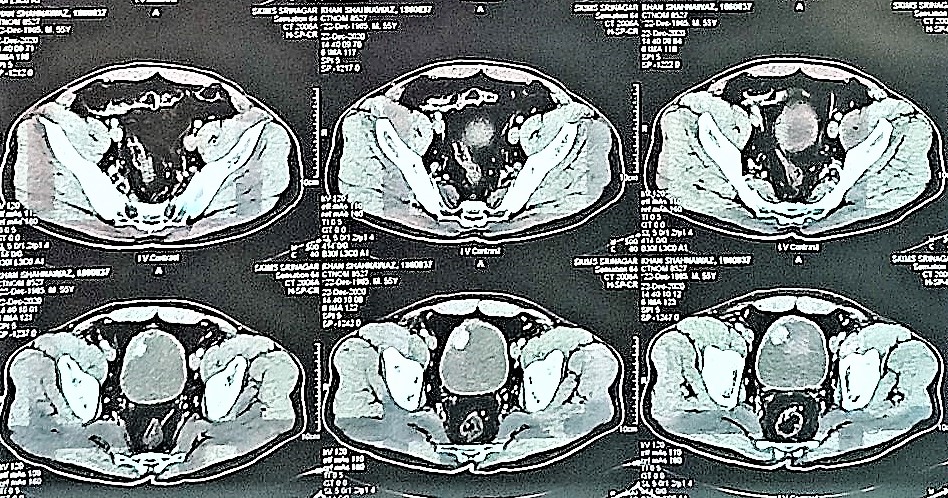
Non-contrast computed tomography (CT) scan of the pelvis showed eccentric thickening of the anterior wall of the bladder of size 5.1x2.6 cm, it was reported as suspicious for carcinoma (Figure 1).
There was also a history of a large vesicle calculus (or multiple coalescent calculi) in the past. Also noted was severe right-sided hydronephrosis with hydroureter due to a right ureteric calculus. A transurethral biopsy was performed at the site of the thickening of the bladder wall.
|
|
|
Figure 1. Non-contrast CT scan of the pelvis showing eccentric thickening of the anterior wall of the bladder. |
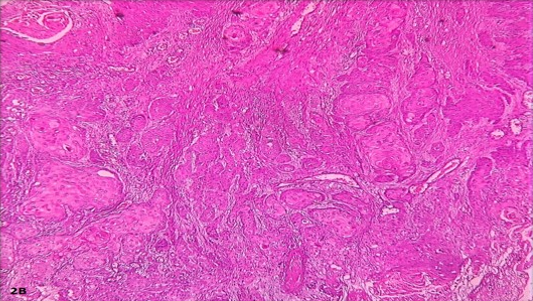
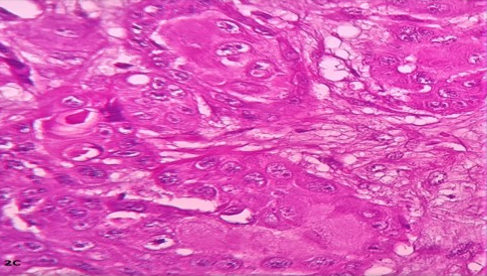
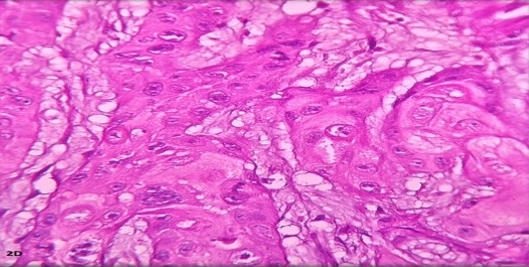
The biopsy specimen was received as multiple tissue fragments gray, and white. Tissue sections showed a malignant tumor composed of moderately pleomorphic cells arranged in nests and cords. The tumor cells showed vesicular nuclei with prominent nucleoli and ample eosinophilic cytoplasm. Many keratin pearls were noted along with scattered mitoses. The same picture was observed in all the tissue bits sampled (Figures 2a-2d).
|
|
|
|
a) |
b) |
|
|
|
|
c) |
d) |
|
Figure 2. a) Photograph showing multiple tissue fragments gray, and white. b) Photomicrograph showing malignant tumor composed of moderately pleomorphic cells arranged in nests and cords. H&E×20. c) Tumour cells with vesicular nuclei and prominent nucleoli along with abundant eosinophilic cytoplasm. H&E×40. d) Photomicrograph showing scattered atypical mitotic figures. H&E×40 |
|
A diagnosis of well-differentiated primary SCC of the urinary bladder was made. The patient was evaluated and deemed unfit for radical cystectomy and hence preferred course of the treatment plan was TURBT followed by concurrent radiotherapy.
Results and Discussion
Bladder stones are more common in the elderly. Males are affected three to four times more than females. The common signs of this disease are recurrent urinary tract infections, urinary retention, and hematuria.[1, 9]
SCC of the urinary bladder is an uncommon malignancy that accounts for 1-3 % of all bladder malignancies. The average patient usually is an elderly male. The major contributing cause of bladder cancer is chronic inflammation. This is usually consequent to chronic urinary tract infections, bladder stones, and schistosomiasis. This results in squamous cell metaplasia of the bladder urothelium, followed by dysplasia which may progress to the development of SCC.[1, 9, 10]
The bladder cancer known as SCC is extremely rare. Postulated causes of non-bilharzial SCC include bladder calculus, persistent indwelling urinary catheter, chronic urinary tract infection, and foreign materials.[7] Our patients' histories included prior recurrent urinary tract infections. In our case, no other etiological factors for pathogenesis could be identified. Hematuria is the most common painless clinical sign of bladder SCC. Other unusual presentations include urinary blockage and signs of an irritable bladder.[7] On urine examination, our patients revealed hematuria. He was also experiencing painful micturition and decreased frequency. SCC can be categorized as being well, moderately, or poorly differentiated based on histology.[7] A comprehensive sample is required to distinguish the SCC of the bladder from TCC with squamous differentiation.[7, 9] The patient's bladder tumor was removed transurethral, and the whole material was examined to rule out any TCC foci, leading to the diagnosis of primary SCC. A comprehensive systemic assessment of both instances ruled out the presence of any metastatic SCC. The majority of bladder SCC are high-grade, aggressive, exhibit involvement of the muscles, and have a bad prognosis.[1, 8, 9] Muscle involvement and a high-grade diagnosis were made for our instance. The ideal Approach to management and prognosis in SCC bladder is still uncertain due to the limited number of studies as a result of the shorter database. Also, most cases present late, and fewer can withstand the full treatment. Radical Cystectomy with urinary diversion is the gold standard treatment for SCC and has a higher 5-year survival rate compared to other modalities including partial cystectomy, radiotherapy, and chemotherapy, however rate of recurrence is still high.[11]
Neoadjuvant or adjuvant therapies (radiotherapy or systemic therapy) are thought to reduce recurrence and increase survival.[11] After receiving the first round of radiation, our patient was unable to handle the adverse effects and eventually passed away.
Conclusion
SCC of the bladder is an extremely rare kind of cancer (1-3%). Chronic inflammation is a big risk factor for this particular kind of bladder cancer. There have been reports of several SCC histological variations. Since their clinical prognosis and therapy differ from TCC, identification of this unusual form is crucial for improved management of these individuals.
None.
None.
None.
|
||||||||