Deniz Publication
Clinical Cancer Investigation Journal
ISSN Print: 2278-1668, Online: 2278-0513
ISSN Print: 2278-1668, Online: 2278-0513
Statistical Data (1978-2020) on Prostate Cancer in the Southern Population of Mexico
Lauro Figueroa-Valverde1*, Marcela Rosas-Nexticapa2, Magdalena Alvarez-Ramirez2, Maria Lopez-Ramos2, Virginia Mateu-Armand2, Tomas Lopez-Gutierrez1
1Pharmacochemistry Research Laboratory, Faculty of Biological-Chemical Sciences, University Autonomous of Campeche; Humberto Lanz Cárdenas s/n, Ex Hacienda Kalá, C.P. 24085, Campeche, Mexico. 2Nutrition Laboratory, Faculty of Nutrition, University of Veracruz, Medicos y s/n Odontologos 910210, Unidad del Bosque, Xalapa, Mexico
Abstract
Prostate cancer is the main risk factor that increases mortality in men worldwide. Recently, the National Institute of Statistics and Geography of Mexico reported the percentage of mortality from prostate cancer in men of 10.89/10,000 (60 and > 60 years) for patients with this clinical pathology in 2020. This research aimed to evaluate statistical data on prostate cancer in the southern population of Mexico. Mortality rates in southern Mexico were evaluated in 23,527 men with prostate cancer in 1979-2020 years using some data sources such as GLOBOCAN 2020, the Information System of the Mexican Ministry of Health, Google Scholar, and PubMed. The data showed that mortality in patients with prostate cancer in Veracruz City was higher (2018) compared to Campeche (219), Chiapas (977), Guerrero (724), Oaxaca (1356), Quintana Roo (623), and Yucatan (603). The results showed that aging is a risk factor for developing prostate cancer. Besides, this phenomenon could be conditioned through increases in the population of each Mexico city.
Keywords: Prostate, Cancer, Mortality, Mexico
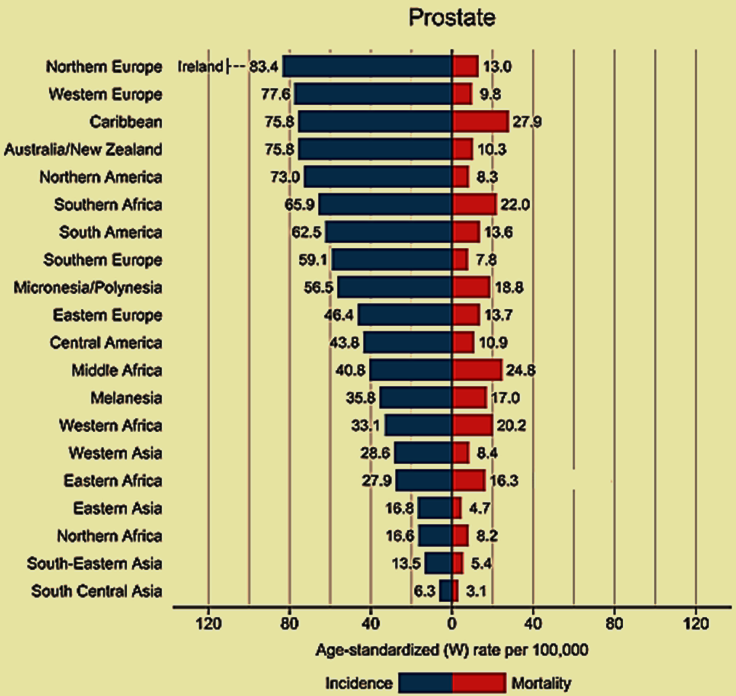
Cancer is one of the main causes of death worldwide, which translates into a decreased life expectancy of the population.[1-6] This clinical pathology has been increasing in both developed and developing countries due to various factors involved such as aging and population growth.[7-10] Here it is important to mention that there are differences in the type of cancer present in each country; In this sense, GLOBOCAN[11] recently reported that in 2020, there was an increase in new cases of cancer in a population of 9,227,484 in women, among which the prevalence of 24.5% (2,261,419 patients) stands out in breast cancer and 9.4% (865634 patients) in the colon and rectal cancers. Regarding the male population (10065305 patients), the prevalence was 14.3% (143594 patients) in lung cancer and 14.1% (1414259) in prostate cancer. Besides, some data indicate that prostate cancer incidence has notably increased in Europe and Northern America compared with Central America and other continents (Figure 1).[11]
|
|
|
Figure 1. Age-standardized (world incidence) and mortality rates, prostate cancer. Source: GLOBOCAN 2020.[11] |
Regarding North America and specifically the United States,[12] some reports show an incidence of new cases of prostate cancer (268,490) and 12.84% of deaths (34,500) in the year 2022. In addition, recently a study displayed that there was an increase in the incidence and mortality of prostate cancer in Canada during 1992-2010.[13] Another data showed that 170,640 Hispano-Americans in the US-Mexico border regions were identified with prostate cancer.[14] Another study carried out in Merida-Mexico showed 532 patients with prostate cancer (ASR 29.8) using CanReg5
software, age-standardized incidence rates (ASR/100,000 person-years).[15] In addition, a report on the burden of cancer in Mexico (1990-2013) showed 29,428 prostate cancer patients, of whom 6,520 died.[16] Another study carried out in a population of 32,349 patients with prostate cancer in Mexico in 1980-1995 showed a higher standardized mortality ratio in Baja California Sur (183.28) compared to cities in southern Mexico such as Campeche (83.27), Chiapas (83.60), Guerrero (57.69), Quintana Roo (47.87), Oaxaca (60.49), Veracruz (80.72) and Yucatan (97.23).[17] All these reports indicate variations in mortality from prostate cancer in Mexico; for this reason, more statistical data is required on this clinical pathology to make a good diagnosis and adequate treatments for its control. Analyzing this hypothesis, the objective of this study was to evaluate the data generated in relation to the total deaths from prostate cancer in southern Mexico from 1979 to 2020.
Materials and Methods
The status of incidence and mortality rates of prostate cancer in 2020 was analyzed by obtaining data from several countries or territories from the GLOBOCAN 2020.[11] Besides, statistical data on prostate cancer in Mexico was through the information system of the Health Secretary of Mexico.[18] Other sources of information such as Google Scholar and PubMed were used to describe some prostate cancer statistics.
Results and Discussion
The results shown in Table 1 indicate that Colima (1771, 7.54%), Mexico City (1036, 4.4%), Guanajuato (1277, 5.43%), Hidalgo (2188, 9.31%), Jalisco (1074, 4.57%), and Nayarit (1357, 5.77%) had the highest mortality and incidence due to prostate cancer problems compared with other Mexico cities. The results showed an increase in prostate cancer in patients with 65 and > 65 years in the following regions such as; the State of Mexico, Michoacán, Jalisco, and Querétaro, compared to other cities in central and northern Mexico.
Table 1. Mortality values of prostate cancer in central and north Mexico from 1979-2020 years. |
||
|
City |
45 to 64 years |
65 and > 65 years |
|
Aguascalientes |
11 |
200 |
|
§N. B.C. |
308 |
27 |
|
¥N. B.C. |
2 |
70 |
|
Coahuila |
27 |
522 |
|
Colima |
5 |
130 |
|
Chihuahua |
47 |
570 |
|
Mexico City |
131 |
1638 |
|
Durango |
22 |
309 |
|
Guanajuato |
49 |
985 |
|
Hidalgo |
18 |
515 |
|
Jalisco |
58 |
1216 |
|
Mexico State |
155 |
2029 |
|
Michoacan |
52 |
1022 |
|
Morelos |
19 |
464 |
|
Nayarit |
15 |
285 |
|
Nuevo Leon |
23 |
647 |
|
Puebla |
58 |
1298 |
|
Queretaro |
15 |
269 |
|
San Luis Potosi |
36 |
732 |
|
Sinaloa |
34 |
498 |
|
Sonora |
20 |
416 |
|
Tamaulipas |
36 |
612 |
|
Tlaxcala |
4 |
279 |
|
Zacatecas |
14 |
487 |
§N. B.C. = North Baja California.
¥N. B.C. = South Baja California.
Source: Health Secretary, General Directorate of Health Information. http://sinaiscap.salud. gob.mx:8080/DGIS/
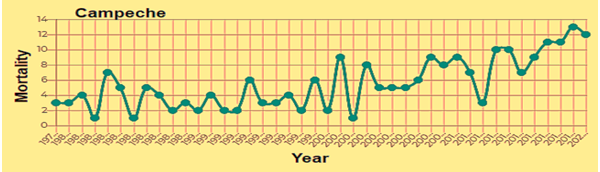
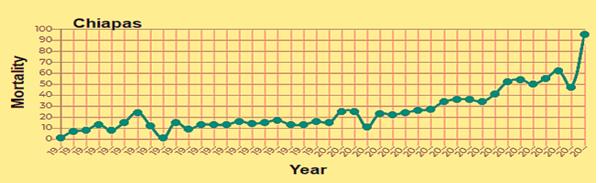
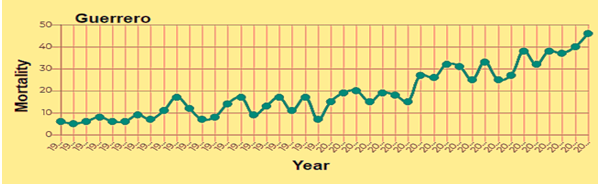
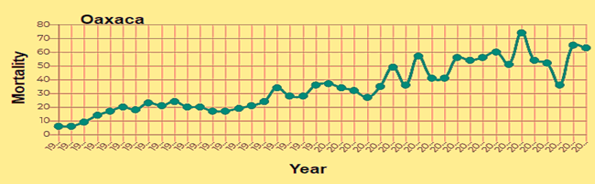
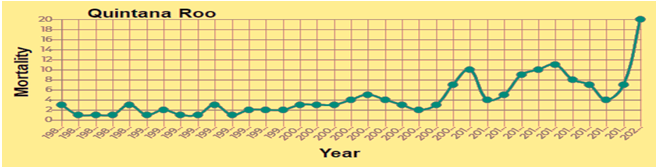
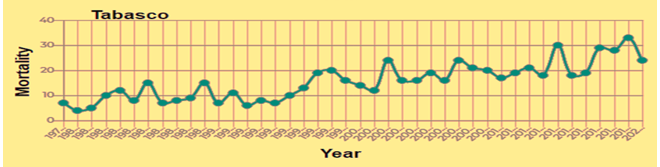
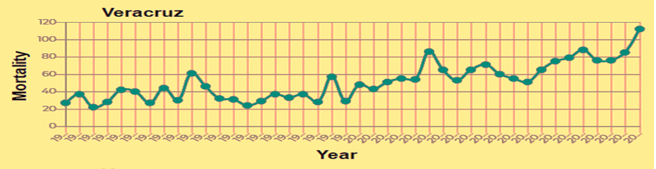
This phenomenon could be due to several risk factors, such as a lifestyle that involves a diet high in saturated fat. [19-23] This hypothesis is supported by some reports; indicating that prostate cancer is related to increased fat intake.[24] For example, a prospective population study of 25,708 Norwegian men showed that a high-fat diet may be a risk factor to produce prostate cancer.[25] Furthermore, prostate cancer in a population of 4,577 men was associated with fat intake as a risk factor that increases mortality.[26] However, contrary to these reports, a study that included 37,349 cases showed that fat intake is not linked to prostate cancer.[27] Analyzing these and other reports suggests that, prostate cancer rates vary substantially by race, ethnicity, geography, and hormonal levels.[28-34] Therefore, these factors could determine the mortality degree of prostate cancer patients in central and northern Mexico cities. Analyzing these reports, alternative research was carried out on prostate cancer in the Southern population of Mexico using the information system of the Health Secretary of Mexico.[18] The Statistical data (1979-2020) shown in Table 2, and Figures 2 and 3 indicate that mortality is higher in patients with 65 and > 65 years in the Chiapas, Veracruz, and Oaxaca cities. However, in Tabasco City, the mortality is higher in patients with 45-64 years.
Table 2. Mortality percentage of prostate cancer in South Mexico from 1979 to 2020 years |
||
|
City |
45-64 years |
65 and> 65 years |
|
Campeche |
13 |
219 |
|
Chiapas |
73 |
977 |
|
Guerrero |
64 |
724 |
|
Oaxaca |
74 |
1356 |
|
Quintana Roo |
156 |
150 |
|
Tabasco |
655 |
623 |
|
Veracruz |
132 |
2018 |
|
Yucatan |
22 |
603 |
Source: Health Secretary, General Directorate of Health Information. http://sinaiscap.salud. Gob.mx:8080/DGIS/
|
|
|
|
|
|
|
|
|
Figure 2. Statistical data on prostate cancer Campeche, Chiapas, Guerrero and Oaxaca from 1979 to 2020. Source: Health Secretary, General directorate of Health information. http://sinaiscap.salud.gob.mx:8080/DGIS/ |
|
|
|
|
|
|
|
|
|
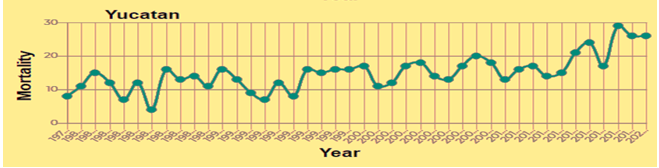
Figure 3. Statistical data on prostate cancer Quintana Roo, Tabasco, Veracruz and Yucatan from 1979 to 2020. Source: Health Secretary, General directorate of Health information. http://sinaiscap.salud.gob.mx:8080/DGIS/ |
These reports suggest that the higher age of the population is one of the risk factors for developing prostate cancer. These studies are supported by other studies which show a direct relationship between age and prostate cancer.[35-40] However, the differences in mortality degree from prostate cancer in each city could depend on other factors such as the size of the population sample involved in each study or the lack of early detection of this clinical pathology, mainly in the rural areas of each region; resulting problems in the registry or information about prostate cancer in Mexico, which can generate difficulties in diagnostic certainty. In this sense, the statistical data generated by the health sector in Mexico are very important to try to establish a good diagnosis in the population for the control of this clinical pathology.
Conclusion
This study reports statistical data on the incidence and mortality of prostate cancer in South Mexico. The results showed that aging is a risk factor for developing prostate cancer. Besides, this phenomenon could be conditioned through increases in the population of each Mexico city.
None.
None.
None.
None.
|
||||||||