Deniz Publication
Clinical Cancer Investigation Journal
ISSN Print: 2278-1668, Online: 2278-0513
ISSN Print: 2278-1668, Online: 2278-0513
Hypofractionated Accelerated Radiotherapy with Concurrent Chemotherapy Versus Conventional Fractionation for LAHNSCC Using IMRT/VMAT: A Pilot Study
Ehab Saad1*, Maha Kamaleldin2, Asmaa Zaghloul1, Emad Habib1, Karim Mashhour1
1Department of Clinical Oncology and Nuclear Medicine, Cairo University, Egypt. 2Department of Medical Physics, Kasr Al-Ainy School of Medicine, Cairo University, Egypt.
Abstract
In fast-growing tumors such as locally advanced head and neck cancers (LA-HNC), hypofractionation effectively overcomes tumor repopulation. We aimed at evaluating the safety and efficacy of moderately hypofractionated radiotherapy with concurrent cisplatin in comparison to the conventional concurrent chemoradiotherapy (CCRT) in LA-HNC. Fifty-four patients with LA-HNC were randomized to receive either: 70Gy in 35 fractions in 7 weeks concurrently with weekly cisplatin 40 mg/m2 (Arm A), or 55Gy in 20 fractions in 4 weeks concurrently with weekly cisplatin 35mg/m2 (Arm B). Volumetric modulated arc therapy/ Intensity-modulated radiotherapy (VMAT/IMRT) plans were done for both arms. Local control (LC), acute toxicity, and progression-free survival (PFS) were recorded and compared between both arms.
A total of 34 patients were in arm A versus 20 patients in arm B, with a median follow-up period of 14.2 months (range 5.1-43.6 months). There was no significant difference in LC, PFS, or acute toxicity between both arms. Complete response occurred in 52.9%(18/34) and 45 %(9/20) in arm A and arm B respectively. In LA-HNC, moderate hypofractionation concurrently with cisplatin appears to be safe and feasible and is associated with a comparable response rate, PFS, and acute toxicity with conventional CCRT protocol.
Keywords: Concurrent chemoradiation, Locally advanced head and neck cancer, Hypofractionated radiotherapy, VMAT, IMRT
The development of radiotherapy over recent years has reintroduced hypofractionation for many tumor sites with comparable disease outcomes to those of conventionally fractionated radiotherapy schedules.[1]
Hypofractionated radiotherapy uses a smaller number of sessions with a larger dose per session which results in reducing of overall treatment time in comparison to a conventional radiotherapy protocol.[2]
In locally advanced head and neck carcinoma, concomitant chemoradiotherapy improves the local control and overall survival (OS) compared with radiation therapy alone.[3]
Recent radiotherapy technologies such as IMRT and VMAT are capable of reducing toxicities related to treatment when compared to conventional treatment.[4]
Patients treated in low-income countries are supposed to have limited resources for radiotherapy and have longer waiting lists than usual to be treated.[5] Therefore, in addition to the theoretical radiobiological and clinical values of accelerated radiotherapy, hypofractionation regimens seem to be an important method to reduce treatment times and thus increase access to radiotherapy.
Treatment of LA-HNC with hypofractionated radiotherapy concurrent with cisplatin was found to be feasible, safe and showed a good response rate which suggests the potential benefit of hypofractionation for LA-HNC, especially for low and middle-income countries, where access to radiotherapy is poor.[1]
The recommendations coming from Risk-Adapted H&N Cancer Radiation Therapy in the COVID-19 era published by the ASTRO-ESTRO consensus statement provided a strong agreement about hypofractionation.[6] Moderately
hypofractionated radiotherapy prescription for head and neck carcinoma, delivering 55Gy in 20 fractions aiming at (2.75Gy per fraction) for 5 days per week, has been offered in Birmingham/Edinburgh.[7] The calculated biologically effective dose (BED) for the hypofractionation is approximately the same as conventional fractionation.[8]
This study was conducted during the period from January 2019 to January 2022. Fifty-four patients with the diagnosis of locally advanced head and neck squamous cell carcinoma (HNSCC) as in (Stage II B, III, IVA, and IVB), who fulfilled the criteria of definitive concurrent chemo-radiation were recruited.
All patients were immobilized in the supine position using thermoplastic head and neck masks. All patients were CT-scanned from the beginning of the skull vertex to the end of the sternum, with 0.3cm CT slice thickness with injected intravenous contrast. The acquired CT images were then sent to the treatment planning system.
The following target volumes were defined based on and according to International Commission on Radiation Units (ICRU) report 50 as well as the supplement of ICRU 62 and 83 guidelines. The Gross target volume (GTV) included primary lesions and clinically significant lymph nodes by reviewing the available CT- and MRI and/or PET-CT.
The primary clinical target volume (CTV) is composed of GTV gross disease with a 0.5 cm margin to cover the microscopic spread of the disease, according to published DAHANCA, EORTC, HKNPCSG, NCICCTG, NCRI, RTOG, and TROG consensus guidelines. A third CTV low-risk sub-clinical disease may be countered.
The Planning treatment volume (PTV) was generally 0.5 cm margin from CTV. The following risk organs were contoured on all CT cuts: Brain stem, spinal cord, Optic chasm, optic nerves bilaterally, bilateral cochleae, bilateral eye globes, both lenses, both parotids, non-involved Oral cavity, larynx, and the mandible and temporomandibular joint, if not laryngeal cancers.
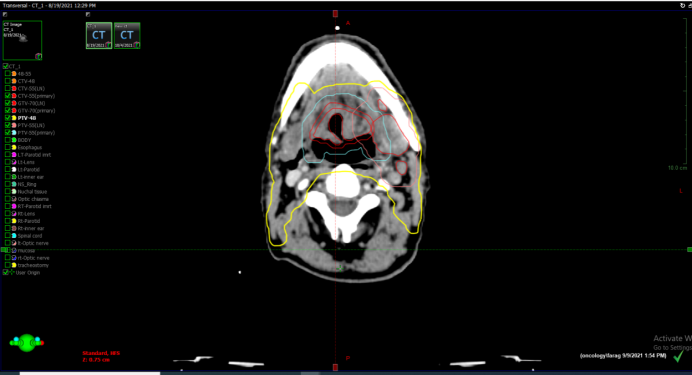
VMAT and IMRT plans were done for all patients. Arm A included 34 patients who received 6MV photons beam by a linear accelerator (DBX VARIAN), 5 fractions per week, to a total of 7 weeks duration (47 days). The dose prescribed was 70Gy in 35 fractions (2Gy per fraction) to the PTV margin of the GTV including both the primary and draining lymph nodes, 60Gy to the PTV of the CTV high-risk, and 54Gy to the PTV margin of the low-risk CTV volumes. The administrated chemotherapy was cisplatin 40mg/m2 weekly regimen (Conventional CCRT) while Arm B included 20 patients who received 6MV photons beam, 5 fractions per week, with a total treatment duration of 4 weeks (26 days). The dose prescribed to the PTV margin of the primary or nodal gross target volume was 55Gy in 20 fractions at 2.75Gy per fraction, 48Gy to the PTV margin of the CTV high risk and 44Gy to the PTV of the CTV low-risk volumes. The chemotherapeutic agent was cisplatin 35mg/m2 on weekly basis (Hypofractionation) (Figure 1).
|
|
|
Figure 1. A case of locally advanced laryngeal cancer case using the hypofractionated protocol (PTV 55 in red and PTV 48 in yellow) |
VMAT and 7 to 9 fields IMRT plans were generated using a 6MV X-ray system. Plan optimization was done using Progressive Resolution Optimizer II implemented in the Eclipse treatment planning system) confirming PTV coverage between 95% and 107%.
The quality of the plans was calculated by Dose Volume Histogram (DVH) data. Both PTV and CTV coverage were evaluated through D2% (the maximum significant dose), D98% (the minimum significant dose), V95%, and V107%. The treatment goal for each patient was to give 95% of the prescribed dose to at least 95% of each PTV.
Restraining doses to other organs at risk was encouraged but should not negatively affect target coverage. The dose constraints for non-critical normal structures listed above were given the lowest priority in the treatment planning process. In case of pre-set targets were not met, clinical judgment was used to decide the best compromise. Acceptance of OAR doses in the two arms was done according to the Quantec model for OAR dose constraints for Arm A and the calculated EQD2 in comparison to 2.75Gy according to the A/B ratio for Arm B (Table 1).
Table 1. Risk organs dose constraints in the 2 arms |
||||
|
|
α/β |
Arm A (70Gy/35fr) |
Arm B (55Gy/20fr) |
Endpoint |
|
Brain stem |
3 |
Mean <54 Gy |
Mean <39.3Gy |
<5% permanent damage |
|
Optic nerve |
3 |
Dmax<54 Gy |
Dmax<39 |
<5% permanent damage |
|
Optic chiasma |
3 |
Dmax<55 Gy |
Dmax<33.9 |
<3% optic neuropathy |
|
Mandible/tempromandibular joint |
<3.5 |
Dmax<70 |
Dmax<62 Gy |
5% osteoradionecrosis |
|
Spinal cord |
<3.3 |
Dmax<50 Gy |
Dmax<33.9 GY |
0.2% myelopathy |
|
Lens |
1.8 |
V18<100% |
V16.98<100% |
50% cataractogenesis |
|
Eye |
3 |
Mean <45 |
Mean <30 Gy |
|
|
Cochlea |
3 |
Mean<=45 |
Mean <=33.9 |
<15%hearing loss |
|
Oral cavity |
10 |
Mean <45 |
Mean < 42.38 |
|
|
One Parotid |
3 |
Mean < 20 |
Mean<18.20 |
<20% salivary function <25% baseline |
|
Both parotids |
3 |
Mean<25 |
Mean <23.58 |
<20% salivary function <25% baseline |
|
Larynx |
3.8 |
Mean< 44Gy Mean<50 Dmax<66 V50<27% |
Mean <42.31 Mean <48.08 Dmax<63.46 V48.08<27% |
<20% edema <30% aspiration <20% vocal dysfunction |
The Common Terminology Criteria for adverse events (CTCAE) was used to assess the acute radiation toxicities. The Response Evaluation Criteria in Solid Tumors (RECIST 1.1)[9] were the reference to evaluate the response just at the end of the 2nd month following the end of radiotherapy, using MRI with contrast.
Statistical analysis
Statistical analysis has been conducted by the use of SPSS 22nd edition, categorical variables are presented in frequency and percentages, and compared using the Chi2 test, quantitative variables were stratified in mean and standard deviation and compared using student T-test for age and baseline body weight between groups, while we used Mann Whitney U test for comparison of weight loss percentage and creatinine clearance among study groups. Survival analysis was conducted using a log-rank test and confirmed using Kaplan-Meier curves. The Cox hazard regression test was conducted to assess predictors for the hazard of progression among study participants. Any p-value <0.05 was considered significant.
Fifty-four locally advanced head and neck cancer patients were recruited in this study, 34 patients in arm A, and 20 patients in arm B, with a median follow-up period of 14.2 months (range 5.1-43.6 months).
The patients’ and tumor characteristics were well balanced between both arms (Table 2).
Table 2. Patients’ characteristics |
||||||
|
|
Group |
P value |
||||
|
Conventional fractionation (n-=34) |
Hypofractionation (n=20) |
|
||||
|
Age in years |
62.2 |
11.9 |
60.4 |
10.1 |
0.571 |
|
|
DM |
No |
30 |
88.20% |
16 |
80% |
0.411 |
|
|
Yes |
4 |
11.80% |
4 |
20% |
|
|
HTN |
No |
28 |
82.40% |
17 |
85% |
0.801 |
|
|
Yes |
6 |
17.60% |
3 |
15% |
|
|
liver disease |
No |
31 |
91.20% |
20 |
100% |
0.172 |
|
|
Yes |
3 |
8.80% |
0 |
0% |
|
|
site |
Hypopharynx |
9 |
26.50% |
3 |
15% |
0.311 |
|
Larynx |
24 |
70.60% |
14 |
70% |
|
|
|
Oropharynx |
1 |
2.90% |
2 |
10% |
|
|
|
Recurrent Larynx |
0 |
0% |
1 |
5% |
|
|
|
Pathology (grade) |
I |
4 |
11.80% |
5 |
25% |
0.438 |
|
II |
23 |
67.60% |
12 |
60% |
|
|
|
III |
7 |
20.60% |
3 |
15% |
|
|
|
T |
T1 |
2 |
5.90% |
1 |
5% |
0.926 |
|
|
T2 |
9 |
26.50% |
5 |
25% |
|
|
|
T3 |
14 |
41.20% |
10 |
50% |
|
|
|
T4 |
9 |
26.50% |
4 |
20% |
|
|
N |
N0 |
3 |
8.80% |
1 |
5% |
0.812 |
|
|
N1 |
23 |
67.60% |
14 |
70% |
|
|
|
N2 |
7 |
20.60% |
5 |
25% |
|
|
|
N3 |
1 |
2.90% |
0 |
0% |
|
Response assessment
Half of the included patients achieved a complete response, 20 (37%) patients reached a partial response, 6 patients (11.1%) had a stationary disease and only one patient reported disease progression (Table 3).
Table 3. Comparison of response rate between study groups |
|||||||
|
|
Group |
Test |
P value |
||||
|
Arm A(n=37) |
Arm B(n=20) |
||||||
|
Count |
Column N % |
Count |
Column N % |
||||
|
Response Rate by MRI |
CR |
18 |
52.90% |
9 |
45% |
X=1.25 |
0.740 |
|
|
PR |
12 |
35.30% |
8 |
40% |
|
|
|
|
SD |
3 |
8.80% |
3 |
15% |
|
|
|
|
PD |
1 |
2.90% |
0 |
0% |
|
|
|
Local control |
No |
4 |
11.80% |
3 |
15% |
X=0.11 |
0.733 |
|
|
Yes |
30 |
88.20% |
17 |
85% |
|
|
There was no statistically significant difference between study groups in terms of response after the different schedules of radiotherapy with a p-value of 0.762.
Toxicity assessment
The highest grade of radiation toxicity was reported for mucositis as grade III was reported in 36 (66.7%) patients and grade IV was reported in 4 (7.40%) patients, followed by skin reaction with grade III in 24 (45.3%) patients, while grade I and II were the most reported grade of radiation toxicity for xerostomia and hematological toxicity accounting for 85.8% and 94.3% respectively.
Five patients (9.3%) patients needed gastrostomy tube insertion.
There was no statistically significant difference between groups based on radiation schedule in terms of the need for gastrostomy, weight loss, baseline weight, and acute radiation toxicities with p-values >0.05 (Table 4).
Table 4. The Assessment of radiation toxicity in both arms. |
||||||
|
|
Group |
P value |
||||
|
Arm A (n=34) |
Arm B (n=20) |
|||||
|
Baseline Body Weight (Kg) |
71.6 |
18.6 |
74.3 |
14 |
0.591 |
|
|
Total weight loss (%) |
10.21% |
1.82% |
9.68% |
2.52% |
0.440 |
|
|
Gastrostomy |
No |
31 |
91.20% |
18 |
90% |
0.885 |
|
|
Yes |
3 |
8.80% |
2 |
10% |
|
|
Mucositis Grade |
Grade 0 |
0 |
0% |
0 |
0% |
0.203 |
|
|
Grade 1 |
0 |
0% |
1 |
5% |
|
|
|
Grade 2 |
9 |
26.50% |
4 |
20% |
|
|
|
Grade 3 |
24 |
70.60% |
12 |
60% |
|
|
|
Grade 4 |
1 |
2.90% |
3 |
15% |
|
|
Skin Reaction |
Grade 0 |
0 |
0% |
0 |
0% |
0.820 |
|
|
Grade 1 |
0 |
0% |
0 |
0% |
|
|
|
Grade 2 |
19 |
55.90% |
10 |
19 |
|
|
|
Grade 3 |
15 |
44.10% |
9 |
15 |
|
|
|
Grade 4 |
0 |
0% |
0 |
0% |
|
|
Xerostomia Grade |
Grade 0 |
0 |
0% |
0 |
0% |
0.784 |
|
|
Grade 1 |
9 |
26.50% |
7 |
9 |
|
|
|
Grade 2 |
20 |
58.80% |
10 |
20 |
|
|
|
Grade 3 |
5 |
14.70% |
3 |
5 |
|
|
|
Grade 4 |
0 |
0% |
0 |
0% |
|
|
Hematological toxicity |
Grade 0 |
2 |
5.90% |
0 |
0% |
0.589 |
|
Grade 1 |
13 |
38.20% |
9 |
47.40% |
|
|
|
Grade 2 |
18 |
52.90% |
10 |
52.60% |
|
|
|
Grade 3 |
1 |
2.90% |
0 |
0% |
|
|
|
Grade 4 |
2 |
5.90% |
0 |
0% |
|
|
Survival analysis
Progression-free survival
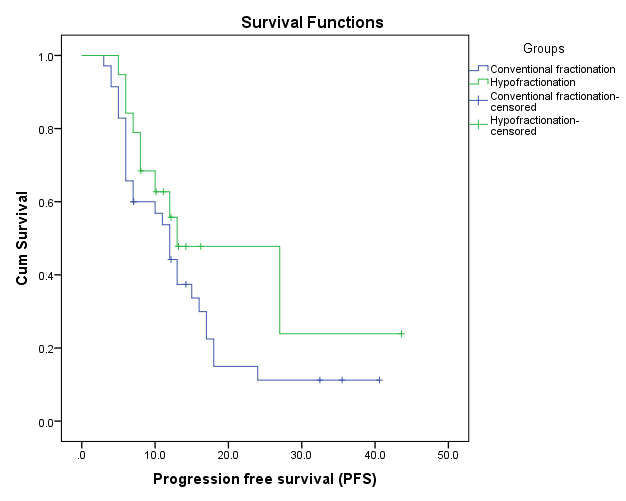
The included patients showed a median PFS of 13 months (95% CI 11.3-14.6).
Oropharynx showed a statistically significant lower PFS (8 months), compared to the larynx (13 months) and hypopharynx (12 months) with a p-value of 0.029.
There was no statistically significant difference in terms of PFS between the arms with a p-value of 0.506 (Figure 2).
|
|
|
Figure 2. Kaplan Meier curve showing PFS according to radiation schedule |
Concurrent chemoradiotherapy remains the cornerstone of the treatment of LA-HNC, providing local control and survival benefit.[10]
Hypofractionation is a notable method for accelerating treatment by minimizing the overall treatment time, the accelerated re-population results are diminished.[11]
There has been increased interest in hypofractionation as it has become the standard of care for localized radiotherapy in different cancers including prostate, breast, melanoma, and rectal cancers. Hypofractionated regimens in LA-HNC weren’t that popular due to the fear of late normal tissue toxicity, even though it has been studied multiple times in the United Kingdom, the data is not very relevant as most of the previous studies did not include advanced treatment planning with IMRT and VMAT, because of using two dimensions (2D) technique. However after adequate administration of IMRT or VMAT, and careful selection of the patients, hypofractionation may turn out to be as effective as standard fractionation, as an appropriate and safe treatment regimen.[12]
Radiobiological view
It’s been suggested that similar log10 cell kill and a lesser late effects BED for the prescribed schedule of 55G given in 20 fractions over 26 days in comparison to the standard fractionated schedule of 70Gy given in 35 fractions over 46 days. With the hypofractionated schedule, the overall treatment time was 26 days. Shortening overall treatment time overcomes accelerated repopulation of tumor clonogens which potentially improves the local control of the disease. With the comparison of late tissues BEDs, the late tissues BED3/2.74 is (105.42 Gy3) in the hypofractionated arm while in the conventional arm with late BED3/2 is (116.7Gy3),[13] which is reassuring regarding late toxicity as it has been always our number one concern when it comes to hypofractionation approach.
Response and survival
The median age of our cohort was 61.5 years with male predominance which coincides with most of the international and national data.[14]
In this study, the CR rate for the whole group of patients was 50% (27/54), demonstrating 52.9% (18/34) and 45 % (9/20) in the conventional fractionation and hypofractionation arm respectively, without any significant difference (P=0.740) in local control between the two groups. The overall response rate (CR, PR, and SD) was 89.5 % in the concurrent conventional arm versus 100% in the hypofractionation arm. One patient developed disease progression after radiation therapy in the conventional arm.
Our results are consistent with the single-arm Brazilian study which enrolled 20 LA-HNC patients. All the patients received 55Gy/ 20 Fr with concomitant cisplatin. They reported a rate of response to both the primary and involved lymph nodes at 95% after 2 months, they stratified the response of the primary lesion and the lymph nodes separately with 85% and 45% respectively.[15]
Another study that followed the Christie scheme, included 158 patients and the treatment plan delivered 3.1Gy in 16 fractions for a total dose of 50 Gy however the radiotherapy technique used was 2D. 45% of the patients had CR while 28% had a partial response, 6% had stable disease, and 21% had progression, 16 out of the 71 patients who achieved CR (22%) progressed with a median DFS of 14 months which is comparable with our results.[16]
In Princess Margaret Hospital group study using hypofractionated radiotherapy 60Gy/25 fr alone versus accelerated RT (70 Gy/35f/6w) with added radiotherapy session on the 1st day of each week in comparison to conventional fractionation chemoradiation, 15% of the patients (N=324) received hypofractionation, they achieved comparable 3-year locoregional control between hypofractionation, accelerated radiotherapy, and CCRT with a median follow up of 4.8 years.
Both grade 3 and 4 late toxicities were less encountered in the hypofractionation arm in comparison to the CCRT group who were treated with conventional fractionation, which is also comparable with our results which showed less grade 3 toxicities in the hypofractionation arm.[17]
In the PET NECK trial, patients with LH-HNC underwent concurrent chemoradiotherapy and were then randomized to surgery where they underwent planned neck dissection versus surveillance by PET-CT; 11% (N= 56) of patients who were treated by 55Gy in 20 fractions. No statistically significant differences were noted in local control of the primary, overall survival and the quality of life at two-year follow-up between the hypo fractionated and conventional fractionation radiation group,[18] which is consistent with our results.
In our study,12 months PFS in the hypofractionation arm is 60% vs 51.4% in the conventional fractionation arm while median PFS in the hypofractionation arm is 14 months versus 12 months in the conventional fractionation arm which is lower than the one reported in the study conducted by Thomson et al. where they reported PFS of 17 months, however, the study enrolled an earlier stage than our cohort where they were six out of the 27 patient had T2 N 0 disease.[19]
Toxicity assessment
The acute adverse effects during radiotherapy were not statistically significant between the two arms and they were numerically comparable with a slight decrease in the percentage of grade 3/4 toxicities in the hypofractionation arm.
Our results revealed that acute skin toxicity G3 was 40% in the investigational versus 44% in the control arm with no G4 skin toxicity encountered in both arms, which is also consistent with the results reported in the Brazilian trial by Jacinto et al. the rate of grade 3 dermatitis was 30%.[1]
Mucositis G3 was 60% in the investigational arm versus 70% in the conventional arm, these numbers are a bit higher than results reported in the systemic review published in 2003 comparing mucositis grade in altered fractionation as the incidence of grade 3/4 mucositis reported were 56%, however the incidence of grade 3/4 mucositis in all studies that discussed hypofractionation was either comparable to our results or associated with higher toxicity, the study conducted by Benghiat et al. in 2014 on 85 oropharyngeal receiving 55Gy/20 fractions concurrent with carboplatin or cetuximab, patients 100% developed G3 mucositis.
In the study conducted by Thomson et al. published in 2015, it included 27 patients with head and neck cancer that received 62.5Gy/25 fractions concurrently with cetuximab, they also reported 78% with grade 3 mucositis.[19]
In another trial conducted in Queen Elizabeth Hospital Birmingham, United kingdom by Meade et al. on 15 patients with oropharyngeal cancer, the patients received 64Gy/25 fractions concurrent either with cisplatin or carboplatin, they reported stage 3 mucositis in 93% of the patients, however, their primary endpoint was the absence of grade 3 toxicity by 3 months.[15]
It should be noted that Egyptian patients could have unique patients characteristics. They have relatively greater tumor volumes with higher stage disease at presentation, with delayed access to health care facilities. This could also possibly explain shorter PFS in our patients. HPV was not assessed routinely differentiating the positive group of patients in our study.
Treatment of LA-HNC patients with hypofractionation concurrently with cisplatin appears to be feasible and safe and provided a good response rate. These data confirm the potential benefit of hypofractionation in LA-HNC, especially in low and middle-economic countries, where access to radiotherapy is poor. Larger randomized trials with relatively longer follow-up periods are needed for further evaluation.
None.
None.
None.
This study was previously approved by our local ethical committee in the department of clinical oncology and nuclear medicine, at Cairo University (reference no. a112018). Informed written consent was signed by each patient prior to their recruitment in our study.
|
||||||||