Deniz Publication
Clinical Cancer Investigation Journal
ISSN Print: 2278-1668, Online: 2278-0513
ISSN Print: 2278-1668, Online: 2278-0513
Anatomopathological and Epidemiological Profile of Granulosa Tumors of the Ovary: About 9 Cases
Imane Boujguenna1*, Fatima Ezzahra Ghlalou1, Anass Fakhri1, Abderraouf Soummani2, Hanane Rais1
1Department of Pathological Anatomy FMFM-UCAM-CHU Mohammed VI-Marrakech-Morocco. 2Department of gynecology FMFM-UCAM-CHU Mohammed VI-Marrakech-Maroc.
Abstract
Granulosa cell tumors are malignant tumors that belong to the tumors of the sexual cords and the stroma. This study permitted us to analyze the granulosa tumors of 9 cases based on the data of the literature. Eight patients presented with adult-type granulosa ovarian tumors and only one patient presented with the juvenile. Patients ranged between ages 29 to 75 age were predominantly postmenopausal women (77.77%). The first conditions found of discovery were tumor syndrome with abdominopelvic pain by the tumor syndrome with abdomino-pelvic pain in first place (77.77%) and abdomino-pelvic masses (55.55%), followed by endocrine syndrome with metrorrhagia (22.22%), and finally signs of dysuria in one patient. On histological examination, the majority of our patients presented a typical microscopic appearance with a tumor proliferation of diffuse architecture with the presence of nuclear grooves in all our patients and Call-Exner bodies in two-thirds. Treatment of these tumors typically involves surgical resection, with the extent of surgery dictated by the stage of disease and the presence of associated comorbidities. Adjuvant chemotherapy and/or radiation therapy may be considered in select cases, but the optimal management strategy for ovarian granulosa tumors remains poorly defined given the rarity of the disease and the lack of large-scale clinical trials.
Keywords: Granulosa tumor, Ovary, Anatomopathological study, Epidemiological profile
Ovarian granulosa tumors are rare malignant tumors belonging to the group of stromal and sex cord tumors.[1] Ovarian granulosa tumors are infrequent malignant neoplasms. They are typified by their indolent course, the high incidence of localized presentation, and their propensity for delayed relapse.[2]
These tumors arise from the sex cord-stromal cells of the ovary and can be either adult or juvenile in nature. Adult granulosa tumors account for the majority of cases and typically present as a unilateral ovarian mass with low malignant potential. In contrast, juvenile granulosa tumors, although rare, tend to be more aggressive and frequently manifest as precocious puberty in young girls.[3]
The clinical course of ovarian granulosa tumors is typically characterized by a protracted disease course, with a tendency towards recurrent disease after prolonged periods of apparent remission. This indolent behavior is often attributed to the presence of well-differentiated cells with low mitotic activity and a low proliferative index.[1]
Treatment of these tumors typically involves surgical resection, with the extent of surgery dictated by the stage of disease and the presence of associated comorbidities. Adjuvant chemotherapy and/or radiation therapy may be considered in select cases, but the optimal management strategy for ovarian granulosa tumors remains poorly defined given the rarity of the disease and the lack of large-scale clinical trials.[4]
We conducted a 10-year retrospective study from January 2010 to December 2019 at the Department of Pathological Anatomy of the CHU Mohammed VI and listed 9 cases of ovarian granulosa tumors. The aim is to study the epidemiological and anatomic-pathological aspect parts of these tumors.
Results and Discussion
Eight patients presented with adult-type granulosa ovarian tumors and only one patient presented with the juvenile. Patients ranged between ages 29 to 75 age were predominantly postmenopausal women (77.77%).
The first conditions found of discovery were tumor syndrome with abdominopelvic pain by the tumor syndrome with abdomino-pelvic pain in first place (77.77%) and abdomino-pelvic masses (55.55%), followed by endocrine syndrome with metrorrhagia (22.22%), and finally signs of dysuria in one patient.
All tumors were unilateral and had a mean an average size of 18 cm. Macroscopically, the solid cystoid appearance was predominant (75%) and hemorrhagic changes were observed in the majority of cases (87.5%).
On histological examination, the majority of our patients presented a typical microscopic appearance with a tumor proliferation of diffuse architecture with the presence of nuclear grooves in all our patients and Call-Exner bodies in two-thirds. The majority of our patients had a mitotic index lower than 10 mitoses/10 fields at high magnification (77.77%).
Immunohistochemical complementation was performed on 3 patients whose most expressed marker was inhibin (100%), followed by calretinin (66.66%) and finally vimentin (33.33%).
The incidence of these tumors is estimated at 1.3 cases/100,000/year. It can occur at any age, but it’s most common around the age of 53. They have a solid component with a multicystic appearance, often encapsulated. The adult form includes five histological subtypes; the most common are microfollicular. The main markers expressed are vimentin (100%), CD 99, and AML (92%). Inhibin is the most intensely positive marker.
|
|
|
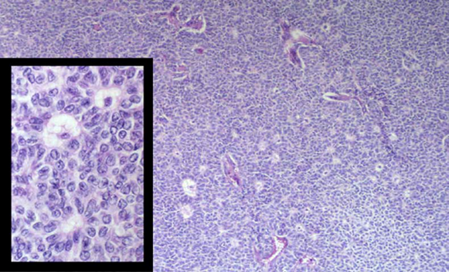
Figure 1. Microfollicular architecture (at x100 magnification), we note in the insert (at x400 magnification), the Call-Exner bodies and the characteristic nuclear grooves |
The incidence of GERD has been estimated by Lauszus et al. to be 1.3 cases/100,000/year.
These tumors arise from the sex cord-stromal cells of the ovary and can be either adult or juvenile in nature. Adult granulosa tumors account for the majority of cases and typically present as a unilateral ovarian mass with low malignant potential. In contrast, juvenile granulosa tumors, although rare, tend to be more aggressive and frequently manifest as precocious puberty in young girls.[3]
GERD can occur at any age, but the adult form occurs primarily around the age of 53 (extremes: 40-70 years) and the juvenile form occurs before puberty or in young women under 30 years of age.[2, 4-6]
The clinical course of ovarian granulosa tumors is typically characterized by a protracted disease course, with a tendency towards recurrent disease after prolonged periods of apparent remission. This indolent behavior is often attributed to the presence of well-differentiated cells with low mitotic activity and a low proliferative index.[1]
Symptoms are variable and include: abdominal pain (30-50%), mass effect bloating, hormonal events such as irregular menstruation, intermenstrual bleeding, postmenopausal bleeding (41%) or amenorrhea.[3]
GERD has a solid component with a multicystic, often encapsulated appearance. On section, the tumor appears yellowish or grayish, with areas of hemorrhage and necrosis. The average diameter is 12 cm (extremes: 1 to 30 cm). It is usually a unilateral tumor.[7]
Adults have 5 subtypes; the most common are micro follicles, characterized by the presence of « Call Exner »; bodies containing eosinophilic, sometimes basophilic fluid, with « coffee bean »; nuclei (Figure 1).[3, 8-10] There is often a reactive proliferation of accompanying thecal cells. Other histological subtypes include macrofollicular, trabecular or insular, and solid tubular. For the juvenile form, the architecture is often lobulated, « Call Exner" » bodies are rare, and signs of luteinization are common.[2]
The main markers expressed by OGT cells are vimentin (100%), CD 99, and smooth actin (92%).
Inhibin is the most intensely positive marker. The other markers are : AE1 AE3 (1/3 of cases), S100
(1/3 of cases) and desmin (65%). Calretinin can be positive but is less specific than inhibin.[11] Granulosa tumors of the ovary are rare tumors. They are characterized by their slow evolution, the frequency of localized stagesan and their tendency to late recurrence.[4, 11] The surgery is the selected treatment for the initial management and recidivisms. The place of the chemotherapy and the adjuvant radiotherapy and the hormonotherapy is badly defined now.
The surgery is the selected treatment for the initial management and recidivisms. The place of the chemotherapy and the adjuvant radiotherapy and the hormonotherapy is badly defined now.
To anyone who has participated in the care of this patient directly or indirectly.
None.
None.
None.
|
||||||||