Deniz Publication
Clinical Cancer Investigation Journal
ISSN Print: 2278-1668, Online: 2278-0513
ISSN Print: 2278-1668, Online: 2278-0513
Should PRIMA Prognostic Index Be Widely Applied Instead of FLIPI2 in the Prognosis of Follicular Lymphoma?
Ngoc Dung Nguyen1, Hai Yen Pham2, Thi Nguyet Anh Phi1, Thi Lan Huong Nguyen3, Minh Phuong Vu2,3*
1Department of Cytology and Histology, National Institute of Hematology and Blood Transfusion, Hanoi, Vietnam. 2Department of Hematology, Hanoi Medical University, Hanoi, Vietnam. 3Hematology and Blood Transfusion Center, Bach Mai Hospital, Hanoi, Vietnam.
Abstract
Recent studies have suggested that PRIMA-PI (Prognostic Index) is a simple tool for predicting patients with follicular lymphoma (FL). With the desire to contribute some experience in the prognosis of FL, we conducted a study to analyze the value of PRIMA-PI versus FLIPI2 (Follicular Lymphoma International Prognostic Index) in the prognosis of FL. Forty-five patients diagnosed with newly follicular lymphoma who received chemotherapy were retrospectively analyzed. All patients underwent bone marrow biopsy to detect bone marrow involvement. Based on histology, the grade was defined according to WHO. The Kapplan-Meyer method and the Cox proportion hazards model were used in the OS (overall survival) analysis to evaluate prognostic indices such as FLIPI2, PRIMA-PI, and the histological classification of FL (grade). According to FLIPI2, the 9-year OS rate of the low-risk group, the intermediate-risk group, and the high-risk group was 100%, 52.9%, and 49.5%; respectively. According to PRIMA-PI, the OS rate for the low-risk group, the intermediate-risk group, and the high-risk group at 9 years was 83.9%, 68.2%, and 43.3%; respectively. According to grade, the 9-year OS rate for grades 1, 2, 3a, and 3b was 83.3%, 73%, 59.3%, and 25%; respectively. Univariate and multivariate analysis showed that only FLIPI2 and grade were truly independent prognostic factors for OS with P=0.03, and 0.012; respectively. On the contrary, we had not yet found the significance of PRIMA-PI in the prognosis of OS, (P=0.056). Caution should be exercised when planning to apply PRIMA-PI widely instead of FLIPI2 in the prognosis of follicular lymphoma.
Keywords: FLIPI2, PRIMA-PI, Histological grading of FL, Grade, Follicular lymphoma, Prognosis
Follicular lymphoma (FL) is a germinal center B cell malignant disease that was considered a slowly progressive tumor. In recent decades there has been progress in its treatment, however, FL still remains incurable.[1, 2] Through this advance, prognostic systems should be changed. FLIPI (Follicular Lymphoma International Prognostic Index) (>60 years of age, <120 g/L hemoglobin, elevated lactate dehydrogenase (LDH), involvement of >4 lymph node regions, and advanced stage of disease) had been developed from data from patients who were treated in the pre- rituximab era.[3-5] With the discovery of rituximab, FL treatment had achieved great success, so FLIPI had been improved to FLIPI2 (>60 years of age, <120 g/L hemoglobin, elevated beta-2 microglobulin, largest lymph node>6 cm and bone marrow involvement), which is more appropriate for the new era with rituximab treatment.[3-5] However, FLIPI has continued to be useful in the post-rituximab era.[3] The genes were interested in finding the new prognostic factor, so m7_FLIPI consisted of FLIPI, and 7 genes were established.[6] However, some studies have shown that it may depend on the type of chemotherapy.[7, 8]
However, the authors also prefer to establish new prognostic systems rather than single factors, so PRIMA-PI (elevated beta-2 microglobulin and bone marrow involvement) was born with the advantage of simplicity. Some authors suggested that PRIMA-PI has sufficient reliability and specificity in the prognosis of FL. Furthermore, PRIMA-PI is not dependent
This was a retrospective cohort study at the National Institute of Hematology and Blood Transfusion, Hanoi, Vietnam. From January 2014 to December 2022, 45 newly diagnosed follicular lymphoma patients who received chemotherapy were retrospectively analyzed.
Before treatment, all patients underwent bone marrow biopsy to detect bone marrow involvement.
Patients were treated with R-CHOP (Rituximab, Cyclophosphamide, Doxorubicin, Vincristin, and Prednisolone) or BR (Bendamustin and Rituximab) for 4-6 cycles and after that received Rituximab maintenance therapy for 2 years.
The diagnosis was confirmed according to WHO 2008 classification of hematopoietic and lymphoid tumors.[18] Based on histology, the grade was defined according to WHO.[3] The stage was classified according to Ann Arbor Stage.[3] The risk classification was defined according to FLIPI2 and PRIMA-PI.[3] Response to chemotherapy was defined according to the criteria of the International Working Group (RECIL 2017).[19]
OS (overall survival) was calculated from the time of diagnosis to the last- follow-up or death. The Kapplan-Meyer method and the Cox proportion hazards model were used in OS analysis to evaluate prognostic indices such as FLIPI2, PRIMA-PI, and grade. P<0.05 was considered a significant statistical difference.
Results and Discussion
This study included 45 patients, with 21 men accounting for 46.7%. The median age of the patients was 56 (range; 27-79 years). The laboratory indices are shown in Table 1. The clinical characteristics of the patients are shown in Table 2. There were 21 patients with bone marrow involvement (BMI) which accounted for 46.7%. Histological features included nodular, para trabecular, diffuse, and mixes with the para trabecular type as the highest frequency.
Table 1. Laboratory indices of the patients |
|||||
|
Index |
N |
Minimum |
Maximum |
Mean |
Std. Deviation |
|
Hemoglobin (g/L) |
45 |
92 |
162 |
125.44 |
15.672 |
|
Platelet (G/L) |
45 |
24 |
932 |
251.31 |
142.718 |
|
WBC (G/L) |
45 |
.46 |
89.21 |
9.2524 |
13.34499 |
|
Neutrophil (G/L) |
45 |
.1104 |
9.8716 |
4.082584 |
2.0788589 |
|
Beta2microglobulin (mg/L) |
45 |
1.16 |
7.42 |
2.7482 |
1.32265 |
|
LDH (U/L) |
45 |
230 |
1013 |
447.22 |
207.917 |
|
Valid N (listwise) |
45 |
|
|
|
|
BMI is an adverse prognostic factor in lymphoma and can be detected in 40% to 70% of patients with FL.[20, 21] The diagnosis of BMI was based on the histology of the bone marrow biopsy pattern. Several studies had compared bone marrow biopsy with flow cytometry (FCM) and PET/CT in the sensitivity for detection of infiltration and have shown that PET/CT may be better, while FCM was more likely to miss.[20, 22, 23]
Table 2. Clinical characteristics of the patients |
|||||
|
Characteristic |
Frequency |
Percent |
Valid Percent |
Cumulative Percent |
|
|
Lymphadenopathy |
No |
3 |
6.7 |
6.7 |
6.7 |
|
Yes |
42 |
93.3 |
93.3 |
100.0 |
|
|
Total |
45 |
100.0 |
100.0 |
|
|
|
Hepatomegaly |
No |
41 |
91.1 |
91.1 |
91.1 |
|
Yes |
4 |
8.9 |
8.9 |
100.0 |
|
|
Total |
45 |
100.0 |
100.0 |
|
|
|
Splenomegaly |
No |
41 |
91.1 |
91.1 |
91.1 |
|
Yes |
4 |
8.9 |
8.9 |
100.0 |
|
|
Total |
45 |
100.0 |
100.0 |
|
|
|
Bone marrow Involvement (BMI) |
No |
24 |
53.3 |
53.3 |
53.3 |
|
Yes |
21 |
46.7 |
46.7 |
100.0 |
|
|
Total |
45 |
100.0 |
100.0 |
|
|
|
Histological Features of BMI
|
Nodular |
5 |
11.1 |
23.8 |
23.8 |
|
Paratrabecular |
9 |
20.0 |
42.9 |
66.7 |
|
|
Diffuse |
3 |
6.7 |
14.3 |
81.0 |
|
|
Mixes |
4 |
8.9 |
19.0 |
100.0 |
|
|
Total |
21 |
46.7 |
100.0 |
|
|
|
Ann Arbor Stage |
IIA |
5 |
11.1 |
11.1 |
11.1 |
|
IIB |
2 |
4.4 |
4.4 |
15.6 |
|
|
IIIA |
12 |
26.7 |
26.7 |
42.2 |
|
|
IIIB |
8 |
17.8 |
17.8 |
60.0 |
|
|
IVA |
10 |
22.2 |
22.2 |
82.2 |
|
|
IVB |
8 |
17.8 |
17.8 |
100.0 |
|
|
Total |
45 |
100.0 |
100.0 |
|
|
|
Grade |
Grade1 |
8 |
17.8 |
17.8 |
17.8 |
|
Grade2 |
24 |
53.3 |
53.3 |
71.1 |
|
|
Grade3a |
9 |
20.0 |
20.0 |
91.1 |
|
|
Grade3b |
4 |
8.9 |
8.9 |
100.0 |
|
|
Total |
45 |
100.0 |
100.0 |
|
|
|
FLIPI2 |
Low risk |
15 |
33.3 |
33.3 |
33.3 |
|
Intermediate risk |
18 |
40.0 |
40.0 |
73.3 |
|
|
High risk |
12 |
26.7 |
26.7 |
100.0 |
|
|
Total |
45 |
100.0 |
100.0 |
|
|
|
PRIMA- PI |
Low risk |
21 |
46.7 |
46.7 |
46.7 |
|
Intermediate risk |
11 |
24.4 |
24.4 |
71.1 |
|
|
High risk |
13 |
28.9 |
28.9 |
100.0 |
|
|
Total |
45 |
100.0 |
100.0 |
|
|
The histological grading of follicular lymphoma was classified according to WHO criteria that showed grade 2 represented the highest rate with 53.3%.
Table 3. Treatment Outcome |
|||||
|
Response |
Frequency |
Percent |
Valid Percent |
Cumulative Percent |
|
|
Valid |
PR |
6 |
13.3 |
13.3 |
13.3 |
|
CR |
39 |
86.7 |
86.7 |
100.0 |
|
|
Total |
45 |
100.0 |
100.0 |
|
|
Note; PR: partial response, CR: complete response
FLIPI2 and PRIMA-PI were used to classify the risk level. There was a difference between the two prognostic systems. According to FLIPI2, the highest rate group was the intermediate-risk group. Otherwise, according to PRIMA-PI, the highest rate group was low- risk group. However, there was no statistically significant difference with p=0.287.
Table 3 shows the response to chemotherapy that was assessed before Rituximab maintenance therapy. Almost patients achieved CR (complete response) to chemotherapy with 86.7%. Table 4 shows that the mean OS was 77.43 months. In the BMI group, the nodular BMI type had the shortest OS, but there was no statistically significant difference.
Table 4. Overall survival according to the histological features of bone marrow biopsy |
|||||
|
Type |
Mean (months) |
P |
|||
|
Estimate |
Std. Error |
95% Confidence Interval |
|||
|
Lower Bound |
Upper Bound |
||||
|
No BMI |
85.674 |
8.213 |
69.577 |
101.771 |
0.684 |
|
Paratrabecular |
75.556 |
15.981 |
44.233 |
106.878 |
|
|
Diffuse |
62.500 |
10.253 |
42.404 |
82.596 |
|
|
Mixes |
48.500 |
21.947 |
5.483 |
91.517 |
|
|
Nodular |
31.400 |
5.009 |
21.583 |
41.217 |
|
|
Overall |
77.430 |
7.268 |
63.184 |
91.677 |
|
Note: BMI: bone marrow involvement
Almost no studies were interested in whether the type of BMI was significant in the prognosis of FL. However, Canioni et al. suggested that the ratio of lymphomatous foci (LFo) area to bone marrow biopsy (BMB) size was considered a prognosis factor for survival.[21]
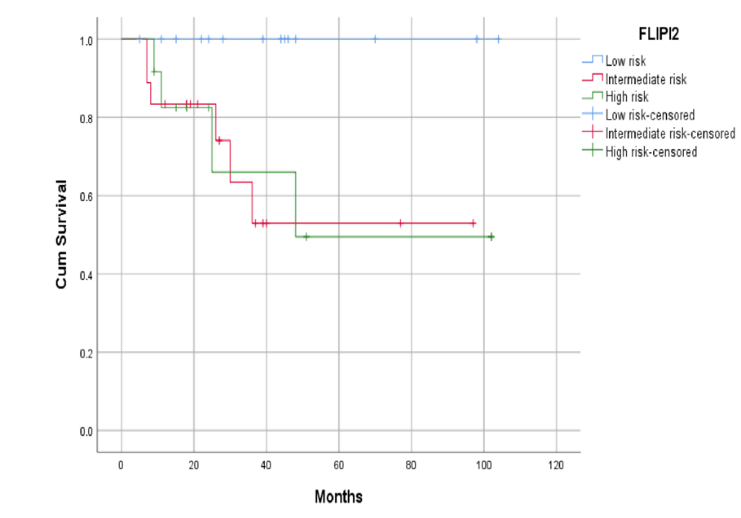
Univariate and multivariate analysis showed that only FLIPI2 and grade were truly independent prognostic factors for OS (Table 5, Figures 1 and 2). On the contrary, we had not yet found the significance of PRIMA-PI in the prognosis of OS (Table 5).
Table 5. Univariate and multivariate analysis prognostic factors for overall survival |
||||
|
Factor |
Univariate analysis |
Multivariate analysis |
||
|
OS (9 years rate) |
P Log-rank value |
P Cox value |
||
|
FLIPI2 |
Low risk |
100% |
0.041 |
0.03 |
|
Intermediate risk |
52.9% |
|||
|
High risk |
49.5% |
|||
|
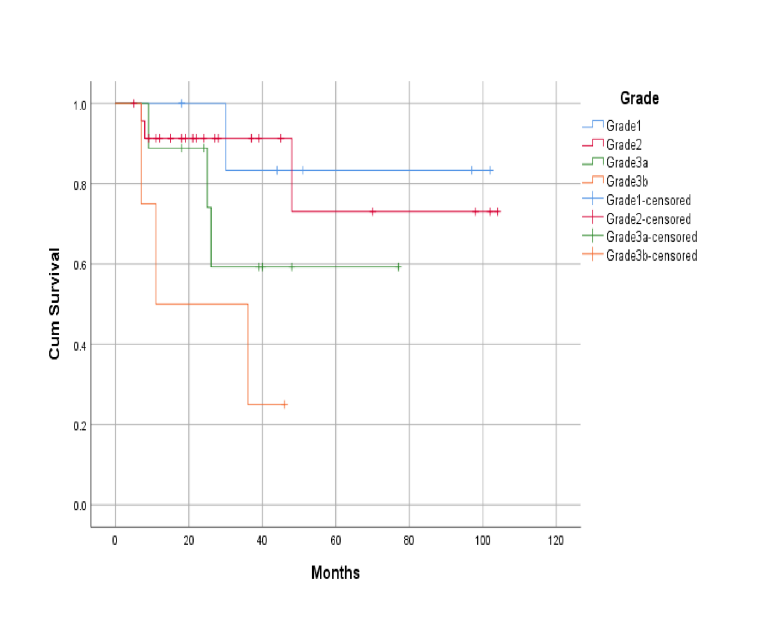
Grade |
1 |
83.3% |
0.041 |
0.012 |
|
2 |
73.0% |
|||
|
3a |
59.3% |
|||
|
3b |
25.0% |
|||
|
PRIMA-PI |
Low risk |
83.9% |
0.056 |
|
|
Intermediate risk |
68.2% |
|||
|
High risk |
43.3% |
|||
The grade is still useful in the prognosis of FL. Studies only showed the difference between grade 3b and the rest. Grade 3b is closely related to DLBCL (Diffuse large B cell lymphoma).[3, 24, 25] However, our study showed a statistically significant difference in the 9-year OS rate between the 4 groups.
|
|
|
Figure 1. OS (overall survival) according to FLIPI2 |
PRIMA-PI is considered a simple prognostic system. Bachy et al. showed that PRIMA-PI was a simplified score system for predicting PFS (Progression-Free Survival) and correlated strongly with POD-24.[16] Alig et al. suggested that PRIMA-PI had the highest specificity to identify high-risk patients compared to FLIPI and FLIPI2.[17] Kimby et al. demonstrated that PRIMA-PI appeared more useful than FLIPI, especially in patients over 60 years of age.[15]
|
|
|
Figure 2. OS (overall survival) according to Grade (Histological Grading of Follicular Lymphoma) |
Mozas et al. suggested that PRIMA_PI was not age-dependent and could identify a high-risk group in older patients, but they also recognized that FLIPI remains the most powerful clinical prognostic index.[26] Wu et al. suggested that FLIPI had the highest positive predictive value, while PRIMA-PI had the highest precision in the analysis of POD-24.[27] Duras et al. showed that there was an overlap between the survival curves of the low and intermediate-risk groups according to PRIMA-PI.[28] According to these studies, PRIMA-PI seems to have specificity for high-risk patients over 60 years of age. Furthermore, almost all of these studies (except for Alig) did not compare PRIMA-PI with FLIPI2. In our study, PRIMA-PI was not significant in OS prognosis, while FLIPI2 and grade were truly independent prognostic systems (with P=0.03 and 0.012; respectively) in the univariate and multivariate analysis.
In general, there is not enough evidence to suggest that PRIMA-PI can replace FLIPI2 in the prognosis of FL. However, it is not easy to rely on only two indices (elevated beta-2 microglobulin and bone marrow involvement) to assess the prognosis of malignant disease. More studies are needed before the widespread application of a new prognostic system. Anyway, whether lymphoma is slow-growing like FL, or fast-growing like DLBCL (Diffuse large B- cell lymphoma), the analysis of prognostic factors is complicated and further studies are still need to find out.[29]
Caution should be exercised when planning to apply PRIMA-PI widely instead of FLIPI 2 in the of prognosis follicular lymphoma.
The authors thank all the doctors and nurses in the Department of H5, National Institute of Hematology and Blood Transfusion, for treating and taking care of all patients in our study.
None.
None.
The Institutional Review Board of National Institute of Hematology and Blood Transfusion waived the need for approval and patient consent because of the retrospective observational nature of the study.
|
||||||||