|
|
|
|
Role of Ki-67 as an Adjunct to Histopathological Diagnosis in the Grading of Astrocytic Tumors
Namita Singh1, Prita Pradhan1*, Ranjana Giri1, Diptiranjan Satapathy2
1Department of Pathology, Kalinga Institute of Medical Sciences, Bhubaneswar, Odisha, India-751024. 2Department of Neurosurgery, Kalinga Institute of Medical Sciences, Bhubaneswar, Odisha, India-751024.
Abstract
The Ki-67 Labelling Index (LI) is used as an ancillary tool to assess cell proliferation activity in glioma diagnosis. It is a potent biologic marker that estimates the growth of neoplasm and thus will aid in identifying the prognosis in patients with glioma. To study the expression of Ki-67 in astrocytic tumors and its correlation with clinicopathological parameters. Clinico-radiological details of forty-three cases of glioma were documented. H&E slides were reviewed for histopathological grade and morphology. KI-67 Labelling Index was studied by immunohistochemical analysis at ‘hot-spot’ areas. Cases were segregated into high and low grades taking 4% as a cut-off as per WHO criteria. Statistical analysis was carried out using standard statistical software with a p-value of ≤ 0.05 taken as statistically significant. A total of 43 patients were included comprising 31 males and 12 females with a mean age of 46.14 years. Ki-67 labeling index showed a statistically significant relationship with the advanced age (p=0.01), higher histological grade (p=<0.00001), presence of cellular atypia (p=0.0002), necrosis (p=<0.00001), and microvascular proliferation (p=<0.00001). Ki-67 assessment supplements standard histopathological grading. It is a simple and reliable method. This study demonstrates that it can serve as an important prognostic marker. It can be used as an adjunct to histopathological diagnosis.
Keywords: Astrocytic tumors, Ki-67, Grade, Atypia
Gliomas are common malignancies of the central nervous system(CNS).[1, 2] Scholzer and Gerdes discovered the Ki-67 antigen in the early 1980s, which expresses two protein variants with molecular weights of 345 and 395 kDa.[3] It is present at all active cell cycle phases (G1,S,G2, and M) but absent in resting cells (G0).[4, 5] In the later stages of mitosis significant decrease in Ki-67 (during anaphase and telophase) levels takes place.[6] The Ki-67protein (pKi-67) expression has been linked to the proliferation of intrinsic cell components in malignant tumors enabling its use as a measure of tumor aggressiveness.[7, 8]
The cell cycle's advancement, changes in cellular distribution, interphase, and process of cell mitosis are all regulated by the expression of Ki-67.[9] Ki-67 is utilized in diffuse astrocytic tumors as a biomarker of tumor cell proliferation that forecasts the biological characteristics of the tumor and the patient's prognosis.[10, 11] Low-grade astrocytomas have a considerably different mean Ki-67 LI compared to anaplastic astrocytomas and glioblastoma.[12]
Evaluation of the tumor's proliferative index (Ki-67) is one such complementary method.[22] Among the many useful biological markers available, the proliferative index provides a quantitative measure of tumor proliferation.[23] Several techniques have been used to calculate the
The study was conducted in the Department of Pathology, over two years between September 2020 to August 2022 after approval from the Institute Review Board as well as Institute Ethical Committee, as per the Declaration of Helsinki. Before, the initiation of the study, informed consent was taken from all the participants whose biopsies were considered for the study. Formalin-fixed paraffin-embedded (FFPE) blocks of histopathologically proven cases of glial tumors were included both prospectively and retrospectively from the archives. Inadequate and poorly-fixed tissues were excluded from the study. After taking informed consent, detailed clinical and radiological information was documented.
Consecutive H&E sections slides were reviewed for histomorphological features including-histological type and grade of tumors, degree of cellularity, atypia, mitosis, presence of necrosis, and microvascular proliferation. Grade I and Grade II tumors were referred to as low-grade tumors, while Grade III and Grade IV were tumors referred to as high-grade tumors. The corresponding sections from paraffin block with a viable tumor in highly cellular areas (including necrosis if present) were chosen for IHC.
IHC for Ki-67 was performed on deparaffinized sections taken on albumin-coated slides using two-step indirect methods. Prediluted ready-to-use Ki-67 monoclonal antibody CAT-P-K001-30 (Clone QR015, Berlin, Germany) was used. Placenta tissue was taken as a positive control. For negative control, the same sections were used by omitting the primary antibody step. The observations were taken independently by two pathologists blinded to the clinical details. The discrepant cases were reviewed and evaluated over a multiheaded microscope with an expert for consensus observations.
A hot spot (area with the highest density of immunostained nuclei) was selected and adjacent fields were counted to include 1000 nuclei. Distinct nuclear staining of tumor cells was recorded as positive. Ki-67 labelling index was recorded as a ‘percentage’ of positively stained nuclei in 1000 tumor cells. The Ki-67 cut-off value given by WHO for glioma is less than 4% for low-grade gliomas and more than or equal to 5% for high-grade gliomas. We categorically divided Ki-67 expression into low and high expression taking 4% as cut off.
For statistical analysis, data were entered into a Microsoft Excel spreadsheet in 2010. Quantitative data were expressed as range, mean±SD, or median. The categorical variables were analyzed using Pearson’s chi-square test or Fisher’s exact test. Statistical analysis was carried out using Microsoft Excel spreadsheet 2010, GraphPad QuickCalcs ©2021 GraphPad Software, and Social Science Statistics©2021 Jeremy Stangroom. A p-value of ≤ 0.05 was taken as statistically significant.
A total of 43 patients were included with a Mean age of 46.14y with M:F=2.5:1. Tumours most frequently involved the frontal lobe (12/43) with 15low-grade gliomas comprising pilocytic and diffuse astrocytoma (11/43) 25% (Figure 1).
|
|
|
a) |
|
|
|
b) |
|
|
|
c) |
|
|
|
d) |
|
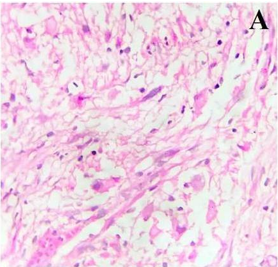
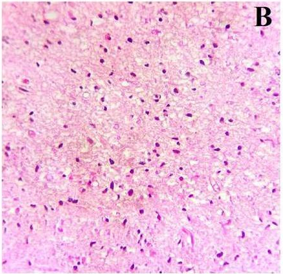
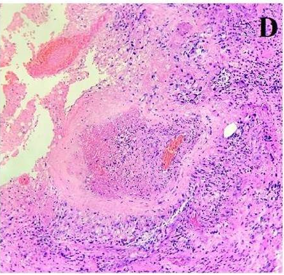
Figure 1. Showing different grades of glial tumors encountered in the study. a) Grade I-Pilocytic Astrocytoma. (H&E,400X); b) Grade II- Diffuse Astrocytoma.(H&E,100X); c) Grade III- Anaplastic Astrocytoma.(H&E,400X), d) Grade IV-Glioblastoma (H&E, 100X) |
The Ki-67 LI was found to be in 95.3% of cases ranging from 0-80% (Mean: 22.65±24.28%) with strong nuclear positivity. Low Ki-67(<4%) was seen in 14 out of 43 cases (32.6%). The correlation of Ki-67 with the clinicopathological parameters is summarized in Table 1.
Ki-67 LI showed a statistically significant relationship with age, histomorphological grade, presence of cellular atypia, necrosis, and microvascular proliferation (Table 1). Higher Ki-67 LI was associated with higher age of the patient, higher histologic grade, and a greater degree of cellular atypia (Figure 2).
Table 1. Correlation of PD-L1 and Ki-67 with clinicopathological parameters |
|||||
|
Sl. No. |
Parameters |
Category (n) |
Ki-67 expression |
‘p’- value |
|
|
Low |
High |
||||
|
1. |
Age (years) |
<46 (19) |
10 |
09 |
0.01 |
|
>46 (24) |
04 |
20 |
|||
|
2. |
Cellularity |
Reduced (27) |
13 |
17 |
0.22 |
|
Increased (16) |
04 |
12 |
|||
|
3. |
Atypia |
Minimal(12) |
09 |
03 |
0.0002 |
|
Marked (31) |
05 |
26 |
|||
|
4. |
MVP** |
Absence (19) |
13 |
06 |
<0.00001 |
|
Noted (24) |
01 |
23 |
|||
|
5. |
Necrosis |
Absence (19) |
13 |
06 |
<0.00001 |
|
Presence (24) |
01 |
23 |
|||
|
6. |
Histologic Grade(WHO) |
Grade I/Grade II (15) |
12 |
03 |
<0.00001 |
|
Grade III/Grade IV (28) |
02 |
26 |
|||
*MVP=Microvascular proliferation.
|
|
|
a) |
|
|
|
b) |
|
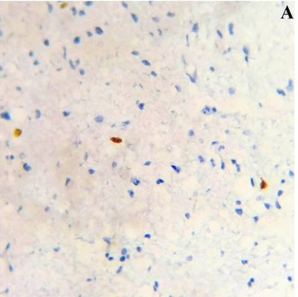
Figure 2. Ki-67LI showing low (<4%) nuclear expression, a) in a case of low-grade glial tumor (Pilocytic Astrocytoma, WHO Grade I) while a case of glioblastoma (WHO grade IV)shows higher (>4%) nuclear staining in b) (IHC for Ki-67, A,B:100X) |
Ki-67 is a biological marker thatis used for grading astrocytoma. It estimates the growth of neoplasm quantitatively as well as predicts the progress accurately. Through qualitative and quantitative estimation of mitosis is important to know the proliferative rate of all tumors but in CNS tumors the mitotic rate is very less and difficult to quantify accurately also. A variety of methods have been used to know the proliferative rate in CNS tumors. Out of these, the most widely used is based on immunohistochemistry with Ki-67. Ki-67 has been established to be a standalone indicator of tumor development and prognosis inglioma patients.[25, 26] HGG (WHO grade III/IV) has a much higher Ki-67 labeling index thanLow-grade glioma (LGG) (WHO grade I/II).[27] Therefore, although histological grade and clinical characteristics are significant prognostic factors in astrocytomas, Ki-67 LI can be utilized in addition to histopathological diagnosis when clinical characteristics and histomorphological grade do not correlate with one another.[10]
Skjulsvik et al. in 2014 studied KI-67 immunostaining in a cohort study of glioma in 267 cases. They observed that Ki-67 expression for high-grade gliomas (grade III/IV) was significantly higher than in low-grade (grade I/II) tumors.[26] Authors who studied the role of immunohistochemical markers p53 and Ki-67 in the grading of glial tumors in a statistically significant rise in Ki67 with grade.[28] Hu et al. in 2013 studied the expression of p53, epidermal growth factor receptor, Ki-67, and O6-methylguanine-DNA methyltransferase in human gliomas and also found that the rate of cell proliferation (Ki-67) increased significantly with the gliomas grade. A statistically significant difference was observed among all WHO grades.[29] Thotakura et al. in 2014 studied the role of the Ki-67 labeling index as an adjunct to the histopathological diagnosis and grading of astrocytomas in cases of astrocytoma and found that mean Ki-67 LI in Grade I astrocytomas was 3.36 ± 4.59 standard deviation (SD), 7.05 ± 4.16 SD in Grade II astrocytomas, 28.24 ± 6.23 SD in Grade III astrocytomas and 38.7 ± 7.19 SD in Grade IV astrocytomas. P values were significant between all grades of astrocytomas except between Grade I and Grade II tumors.[10]
Prior studies have shown that the protein Ki-67 is greatly expressed in glioma cells, however, not in normal brain tissue, therefore, the degree of positive expression increases as the tumor develops.[30] In addition to complementing postoperative pathology in the prediction of tumor biological behavior, the identification of the Ki-67 antigen may be utilized to determine the grade of glioma.[31] Ki-67 is seen in dividing cells and offers an indicator of cellular replication.[30, 32] Tumor progression is facilitated by stem cells which is a part of the epithelial-mesenchymal transition (EMT).[33] Ki 67expression has been documented in stem cells further reinforcing the same.[34] Studies have highlighted that higher Ki-67 in gliomas increases the severity of malignancy. It helps in grading as well as prognostication. Also, solid malignancies are accompanied by chronic inflammation and raised CRP which is associated with high lymphocyte levels.[35] High Ki-67 levels are associated with poor prognosis and may respond to immunotherapeutic intervention.[3] Ki-67 is seen in dividing cells and offers an indicator of proliferation.[30, 36] Studies have highlighted higher Ki-67 in the gliomas increases the severity of malignancy. Prognostic markers are of relevance for glioblastoma, particularly for survival. Few authors who have studied Ki-67 LI in gliomas have found Ki-67 to be associated with an increase in grade, but they did not show a significant association with isocitrate dehydrogenase (IDH) or with survival.[37] However, few authors have correlated the Ki-67 LI with the volume of the edema zone in radiology.[38]
Gliomas, unlike breast cancer, have no screening methods for early diagnosis and treatment.[39] It can be concluded from the present study that the Ki-67 Proliferation index correlates significantly with higher age, higher histological grade, and a greater degree of cellular atypia. Clinical parameters and histopathological grade are important prognostic indicators, however, Ki-67 can be used as an adjunct to histopathological diagnosis where there is discordant among clinical parameters and histopathological grade, especially in small biopsies.
None.
None.
None.
The study was approved by the Institutional Ethics Committee (IEC) and informed consent was taken from all participants (IEC 493 /2020).
|
||||||||