|
|
|
|
Review of the Literature and Current State of Knowledge on the Management of Lung Neuroendocrine Neoplasms
Krzysztof Jurkiewicz1, Michał Miciak1*, Krzysztof Kaliszewski1
1Department of General, Minimally Invasive and Endocrine Surgery, Faculty of Medicine, Wroclaw Medical University, Wrocław, Poland.
Abstract
Lung neuroendocrine neoplasms (LNENs) are lesions originating from diffuse endocrine cells within the bronchial walls and lung parenchyma. In recent years, there have been significant advances in the diagnosis and therapy of these neoplasms. This paper reviews recent developments in these areas, focusing on the latest research and treatment strategies. In the context of diagnosis, new imaging technologies including high-resolution computed tomography (CT), high-resolution and positron emission tomography-computed tomography (PET-CT) imaging, are providing more precise information on tumor spread and evaluation of metabolic activity. Advances in the field of molecular biomarkers allow a more personalized approach to the diagnosis of LNENs. In the therapeutic area, new targeted drugs and immunotherapy are showing promise in the treatment of LNENs. The development of molecular therapies such as tyrosine kinase inhibitors and somatostatin analogs, is opening up new treatment perspectives, increasing the efficacy of therapy, and improving patient quality of life. The paper also focuses on important research directions and clinical advances in the diagnosis and therapy of LNENs, presenting the current state of knowledge about these rare tumors. The conclusions aim to provide a synthetic view of the latest developments in the field, encouraging further research and improving treatment strategies for LNENs.
Keywords: Lung neuroendocrine neoplasms, Neuroendocrine neoplasms, Molecular biomarkers, Imaging techniques, Targeted therapy, Immunotherapy
Lung neuroendocrine neoplasms (LNENs) currently represent about 30% of all neuroendocrine tumors detected and 1-2% of all lung neoplasms. We classify them histologically into four main groups: typical carcinomas (TCs), atypical carcinomas (ACs), large cell neuroendocrine carcinomas (LCNENs), and small cell carcinomas (SCCs).[1, 2] In terms of the differentiation of cells in the tumor, TCs and ACs are well-differentiated tumors. TCs are tumors with low malignancy and long survival, while ACs are tumors with intermediate malignancy and varying clinical behavior. The other 2 groups, LCNECs, and SCCs – are poorly differentiated high-grade tumors with short survival times. These lesions are graded according to mitotic activity, presence of necrosis, and Ki-67 proliferation index.[3, 4] Patients with LNENs present symptoms such as cough, hemoptysis, dyspnea, and chest pain. There is a necessity to closely compare these symptoms with those of typical lung cancers, which can significantly affect the quickness and accuracy of diagnosis.[5] Importantly, LNENs can produce and secrete a variety of substances, such as hormones or neuropeptides which can lead to a variety of clinical manifestations and influence therapeutic strategies.[2] It is also important to note the dependence of symptom severity with increasing tumor stage. The survival rate of patients with LNENs depends on many factors, including tumor type, stage of the disease (Table 1), and effectiveness of the provided treatment. Contemporary advances in diagnostics, including modern imaging technologies and the identification of molecular biomarkers improve the detectability and efficacy of therapy. However, there is still a need for research into new treatment strategies and a better understanding of the biology of these rare neoplasms to enhance the prognosis and patient quality of life.[1]
Table 1. Stage of disease resulting from TNM classification |
|
|
Stage |
Description |
|
0 |
tumor in situ (Tis) |
|
IA |
tumor limited to the lung, size ≤2 cm, without lymph node metastases or distant metastases |
|
IB |
tumor limited to the lung, size >2 cm to ≤5 cm, without lymph node metastases or distant metastases |
|
IIA |
tumor limited to the lung, size >5 cm, without lymph node metastases or distant metastases |
|
IIB |
tumor limited to the lung, size >5 cm, with lymph node metastases, without distant metastases |
|
IIIA |
tumor of any size, with lymph node metastases on the same side, without distant metastases |
|
IIIB |
tumor of any size with metastases to lymph nodes on the contralateral side or the mediastinal space, as well as a tumor of any size with metastases to lymph nodes on the same side but with metastases to lymph nodes on the contralateral side |
|
IV |
tumor with distant metastases, such as metastases to lymph nodes external to the thoracic area or metastases to distant organs |
Materials and Methods
The review was performed based on PubMed, PubMed Central, and Google Scholar online databases. Papers concerning the last 10 years of LNEN's management were taken into consideration. Various forms of the following terms: "lung neuroendocrine neoplasms", "LNEN diagnosis", "lung carcinoid", "neuroendocrine tumor therapy" and "LNEN systematic treatment" were used for research. Original articles and meta-analyses were selected after analyzing abstracts. Of publications from the fields of surgical oncology, clinical oncology, and pulmonology, those that comprehensively described the topic were accepted. Finally, 46 articles have been studied for this paper.
Diagnostics
Imaging techniques for LNENs are based on the same principles, as in non-neuroendocrine tumors of this organ.[6] Computed tomography (CT) is fundamental, with magnetic resonance imaging (MRI) further down the line. The undoubted advantage of CT is the rapid acquisition of high-resolution images, along with the ability to visualize 3D lung structures. In the diagnosis of LNENs, it is recommended to use a CT scanner with a 64-row detector. The use of contrast is also an important aspect of the examination. In most cases, as a result of the prominent vascularization of the thoracic area, tumors are demarcated against solid tissue only in the early arterial phase of imaging.[7, 8] It is strongly advisable in hospitals with access to positron emission tomography-computed tomography (PET-CT) to perform this scan as an early treatment control and assessment of metastasis, due to the highest specificity and sensitivity of this type of imaging. Because of the histological differentiation of the tumors in this group and the tumor proliferation rate, appropriate radioactive agents are used. Atypical lesions, and those with a Ki-67 index greater than 10-20% are better visualized after intravenous administration of 18F-fluorodeoxyglucose.[9, 10] One of the crucial biochemical markers is chromogranin A (CgA), a protein secreted from cells of the diffuse endocrine system. Elevated levels of CgA can indicate the presence and growth of a neuroendocrine tumor. Additional markers, such as synaptophysin, neuron-specific enolase (NSE), or other hormonal substances secreted by specific tumors, can also be considered in the LNEN diagnosis.[11] The role of biopsy remains fundamental in confirming the histological nature of the tumor, as well as in determining the grade of malignancy. It is worth emphasizing that a comprehensive diagnosis, including biochemical, imaging, and histopathological examinations, is essential for the effective planning of treatment strategies and prognosis of the disease process.[12] (Table 2) summarizes diagnostic methods for LNENs.
Table 2. Diagnostic methods for LNENs. |
|
|
Method |
Advantages |
|
CT |
location and size of LNEN, assessment of metastasis to other areas of the lungs and organs, evaluation of the condition of the lymph nodes |
|
MRI |
higher soft tissue resolution than CT, precise analysis of tumor structure, and infiltration of adjacent tissues |
|
PET-CT |
use of labeled fluorodeoxyglucose (FDG) to assess tumor metabolic activity, helping to assess the complexity and malignancy of the tumor |
|
Biochemical tests (CgA, synaptophysin, NSE) |
evaluating the levels of biochemical markers such as chromogranin A (CgA), synaptophysin, or neuron-specific enolase (NSE) |
|
Histopathological biopsy |
crucial for confirming the histological type of the tumor, determination of the grade of malignancy of the tumor, essential for accurate diagnosis |
Therapy
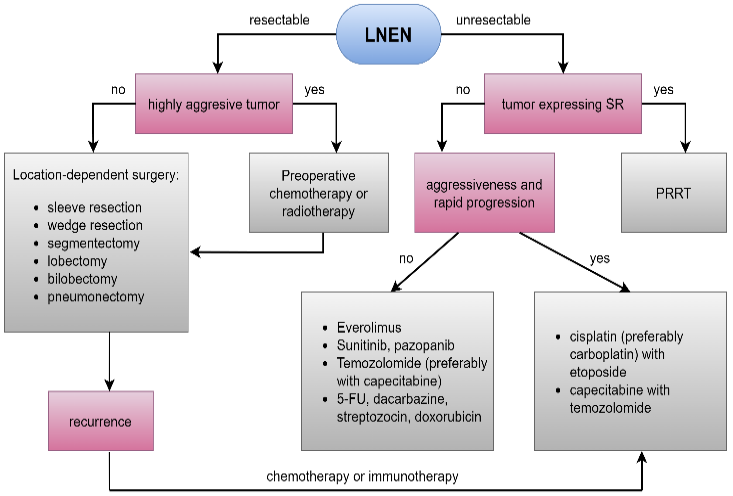
LNEN therapy depends on the location of the tumor. In case of resectability, partial or radical resection of the tumor-affected lung is performed, in addition, chemotherapy and perioperative radiotherapy are used if the tumor presents high aggressiveness. In the case of unresectability, therapy depends on the expression of somatostatin receptors on the surface of tumor cells. When somatostatin analog therapy (PRRT) cannot be used, chemotherapeutic agents or immune agents for LNENs are the last line of treatment.
Surgical treatment
The primary method of treatment is a radical surgical procedure. Its purpose is to completely remove the pathological tissue while preserving the functional integrity of the lung as much as possible. Depending on the location and extent of the LNEN, different techniques are used. For centrally localized TCs, conservative resection, i.e. sleeve resection, segmentectomy, or wedge resection is implemented. For patients with ACs, especially in a peripheral location, lobectomy or bilobectomy is often required, and in extreme cases pneumonectomy.[13, 14] For aggressive tumors, preoperative chemotherapy and/or radiation therapy is strongly recommended.[15] In recent years systematic lymphoadenectomy has been increasingly used alongside surgical treatment. If histopathological examination does not find nodes with malignant lesions, then no follow-up lobectomy is required. However, in patients with metastases in these structures, a lobectomy should be performed with adequate pulmonary reserve.[16, 17] Many authors strongly recommend a follow-up chest CT scan, keeping in mind the risk of recurrence after surgical treatment. The recurrence rate after resection is believed to be about 20% in ACs and 5% in TCs. The testing regimen for a typical carcinoma is as follows: CT at 3 and 6 months, then annually for 3 years.[18, 19] At the same intervals, the patient is required to control the concentration of CgA. Longer imaging and laboratory follow-up are required after resection of an atypical lesion. In this case, CT and CgA should be performed 3 months after surgery and then every 6 months for 5 years.[20]
Systemic treatment
Systemic treatment of LNENs is based on the use of somatostatin analogs as first-line agents.[21] In a study by Öberg et al. administration of these drugs to patients resulted in partial remission in 5-10% of cases, arrest of progression in 30-50%, and symptomatic improvement in 40-60%.[22] It is now believed that in SCCs, therapy with somatostatin analogs is not indicated. The five-year survival rate is less than 5%.[23] A study by Caplin et al. showed that median progression-free survival in LNEN patients after lanreotide administration was 32.8 months.[24] A modification and extension of this therapy is peptide receptor radiotherapy (PRRT) and the use of radio-labeled somatostatin analogs. This method is used as the treatment of choice in LNENs with high levels of somatostatin receptor (SSTR) expression. It shows the best response for a subgroup of large-cell neuroendocrine neoplasms. It has used radio-labeled 90Y-octreotide for many years, and 177LuDOTA-Tyr3-octreotate in recent years. Despite its relatively narrow audience, PRRT can be considered a useful option in patients with progressive LCNEC and strong SSTR expression.[25] Ianiello et al. published a study stating that progression-free survival twenty months after 177Lu-Dotatate was 65.2%, compared to only 10.8% in the control group.[26] Traditional chemotherapy is the gold standard for aggressive LNENs with high growth rates and low SSTR expression. There is no single, generally accepted treatment regimen for these lesions. Monotherapy is recommended for patients who undergo chemotherapy as an adjunctive treatment after surgery. Combination therapies, originally intended for patients with inoperable lesions, are more effective.[27, 28] Turner et al. published the results of treating patients with cisplatin, 5-fluorouracil, and streptozotocin. Partial remission was achieved in 25% of patients and inhibition of progression in 51%. The research group of Bajetta et al. evaluated the efficacy of capecitabine and oxaliplatinin a group of 27 patients. The results showed partial remission in 27.5% of patients and inhibition of progression in 35%.[29] The effect of orally administered temozolomide (TMZ) is also noteworthy. On average, it shows a 23% remission response and 40% tumor growth arrest.[30, 31] Nowadays the role of TMZ as monotherapy has been limited. It has been accepted as a substance that helps to stabilize the disease, but no significant remission is achieved. An exception to its use is the exceedingly rare metastasis from the lungs to the brain. TMZ, as a lipophilic substance, shows a good therapeutic effect in this situation.[24] It is worth noting the significant efficacy of combination therapy of TMZ with capecitabine. The paper of Al-Toubah et al. showed as much as 83.2% benefit with this therapy. This percentage includes disease stabilization and remission combined.[32] According to more recent studies, six cycles of cisplatin with etoposide and subsequent irradiation are particularly recommended. In case of resistance to treatment with first-line chemotherapeutics, the patient should be administered topotecan or a combination of cyclophosphamide, epirubicin, and vincristine.[33] In addition, authors currently advocate replacing cisplatin with carboplatin, due to similar efficacy and minor side effects of therapy. Molecular targeted therapy, as the latest weapon in the treatment of LNENs, is based on the use of tyrosine kinase (TK) inhibitors and mTOR inhibitors. Everolimus is a first-line treatment option in cases of advanced, inoperable LNEN, but is also a reasonable option for further lines of therapy.[34, 35] Also, the use of sunitinib is associated with good response rates. Among the 41 patients studied, 43.9% showed remission of the lesion, and 83.4% showed inhibition of progression. The median survival free from recurrence rate was 10.2 months.[36] Other substances in this group, lenvatinib, and surufatinib, are undergoing efficacy trials for the treatment of LNENs.[37] It is also important to mention a new group of drugs that gives promising results in the treatment, immune checkpoint inhibitors. These are antibodies targeting the programmed cell death ligand receptor (PD-L1). They appear to be ineffective as monotherapy, but the combination of pilimumab with nivolumab has shown activity in patients with neuroendocrine tumors, mainly primary lung tumors. Other substances in this group have not shown promise in studies, but they are underway to combine and be administered in therapy.[38, 39] An example of a management algorithm for a LNEN patient is presented in (Figure 1).
|
|
|
Figure 1. Management algorithm for patients with LNENs. (Abbreviations: LNEN – lung neuroendocrine tumor, SR – somatostatin receptor, PRRT – peptide receptor radionuclide therapy, 5-FU – 5-fluorouracil) |
Conclusion
LNENs are a rare and heterogeneous group of tumors whose advances in diagnostics and therapy present the dynamic direction of medical research. LNEN diagnosis includes a variety of methods, such as CT and MRI, as well as biochemical tests using markers such as CgA. In clinical practice, the combination of different diagnostic methods is essential to accurately determine the stage of the disease. In the therapeutic area, there is a clear direction for individualized strategies, especially in the context of advances in molecular therapy. Innovative targeted drugs and the development of immunotherapies are emerging as promising options for the treatment of LNENs, especially in cases where traditional approaches are unsuccessful. Radical resection with lymphadenectomy remains an important option in the treatment, but an integrated approach that incorporates modern systemic therapies is increasingly being developed. Over the past decade, there have been exceptional advances in understanding the biology of LNENs and in identifying new therapeutic targets. These findings are pushing toward more effective and personalized forms of treatment, with the prospect of improving therapeutic outcomes and patient quality of life. However, further research and clinical experience are needed to clarify the complex nature of these rare neoplasms and improve diagnostic and therapeutic strategies.
We would like to express our gratitude to the Editors and the Reviewers for their work in reading and evaluating our paper.
None.
None.
None.
|
||||||||