Deniz Publication
Clinical Cancer Investigation Journal
ISSN Print: 2278-1668, Online: 2278-0513
ISSN Print: 2278-1668, Online: 2278-0513
Pulmonary Carcinosarcoma is a Rare Cancer with a Poor Prognosis – A Retrospective Study
Abdulrahman Hakami1,2*
1Department of Internal Medicine, Faculty of Medicine, Jazan University, Jazan, Saudi Arabia. 2Department of Pulmonary Medicine, Amsterdam University Medical Center, Amsterdam, Netherlands.
Abstract
Pulmonary carcinosarcoma (PCS) is a rare malignant mixed tumor characterized by a biphasic histopathological pattern of both epithelial and sarcomatous components. It is estimated to account for less than 1% of all pulmonary neoplasms, and patients are predominantly elderly, male, and smokers. The biological behavior and clinicopathological characteristics of PCS are not well documented. This study aimed to address this research gap. This retrospective study included eight patients with a pathologically confirmed diagnosis of PCS. All the patients had a large solid lung tumor, ranging in diameter from 3.5 to 21.5 cm. Six patients had central lesions and two had peripheral lesions. The clinical presentations depended on the localization of the tumor and included mainly cough, dyspnea, and hemoptysis. Complete resection was performed in seven patients. PCS has a highly aggressive nature and a propensity for frequent metastasis, resulting in a poor prognosis and short survival times, ranging between 6 months to 1 year. The use of neoadjuvant and adjuvant chemo-radiotherapy is controversial and not considered fully effective. Surgical lung resection is considered the most effective therapy for this tumor, but even then, survival rates are very low. PCS is a rare and aggressive form of cancer that is difficult to treat. More research is needed to develop better treatments for this disease.
Keywords: Pulmonary carcinosarcoma, PCS, Pathology, Surgery, Prognosis, Survival rate
Pulmonary carcinosarcoma (PCS) is an extremely rare neoplasm of the lung, and accounts for only 0.1%–0.3% of all primary pulmonary neoplasms.[1-3] It was first described by Kika et al. in 1908. In the latest World Health Organization (WHO) classification of lung tumors (in 2021), PCS is classified as a subgroup of sarcomatoid and pleomorphic carcinoma, giant cell carcinoma, pulmonary blastoma, and spindle cell carcinoma.[4, 5] It is characterized by two distinct histological components—an epithelial and a sarcomatous component.[6, 7] PCS occurs predominantly in older men and heavy smokers.[8, 9] The median age at diagnosis is 60–70 years.[10] The clinical manifestations are cough, chest pain, breathing difficulties, fatigue, and weight loss. The most common presenting symptom is a cough, observed in 57% of patients.[11]
PCS is usually detected on chest radiography in routine medical checkups (±37.5% of cases).[12, 13] The median tumor size at detection is 6.2 cm (range 1.2–15.0 cm).[14] The radiographic findings generally consist of a large solitary mass or extensive opacity due to associated obstructive pneumonitis, atelectasis, or large masses.[15] PCS is divided into central and peripheral types.[16, 17] The central lesions are usually slow-growing and locally invasive, while the peripheral parenchymal tumors tend to metastasize early and are more widely invasive.[18, 19]
Recent studies have reported the definitive diagnosis of PCS based on morphologic characteristics and immunohistochemical staining after surgical resection.[19, 20] In the early stages, complete resection is the primary treatment for PCS. Conversely, in advanced stages, palliative chemotherapy is suggested, but the response is poor and most patients die within a few weeks to months from the disease progression.[21, 22]
Materials and Methods
The study was conducted at Amsterdam University Medical Center (AUMC- VUMC) between 1990 and 2018, after
Adult patients diagnosed with PCS were included. Other types of lung cancer were excluded.
Eight patients with a pathologically confirmed diagnosis of PCS were recruited. All the patients underwent routine laboratory studies, respiratory function tests, and radiological investigations. The radiological interventions included chest x-ray, computed tomography (CT) of the thorax, and positron emission tomography (PET). In addition, the patients underwent bronchoscopy, using which a biopsy specimen was obtained. Mediastinoscopy was performed on one patient who had mediastinal lymphadenopathy.
The patients were evaluated according to age, gender, symptoms, diagnostic approaches, pathological findings, surgical methods, and follow-up findings.
All patients underwent clinical and radiological follow-ups. A standard preoperative and postoperative seventh international TNM staging system was obtained for all patients.
Data were extracted, coded, and analyzed using Statistical Package for the Social Sciences (SPSS) version 25. A P-value of 0.05 was used for statistical significance in all tests. Figures were constructed using Kaplan–Meier survival analysis to analyze the outcome in terms of the site, treatment, and stage of the disease.
Results and Discussion
The study included eight patients with PCS; five of the patients were male, and three of the patients were female. All of the patients were smokers. The age range of the study participants was 50–79 years. The most common presenting complaint of the patients was a cough with dyspnea.
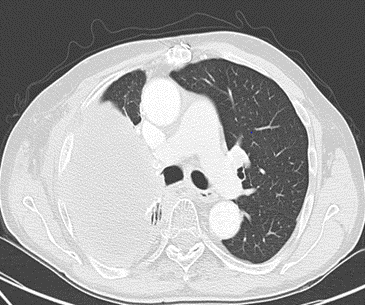
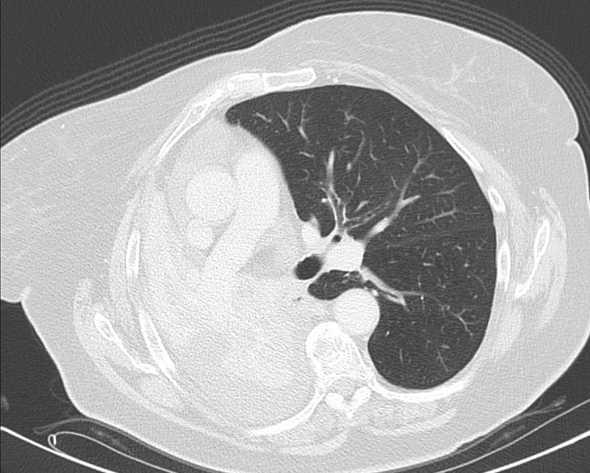
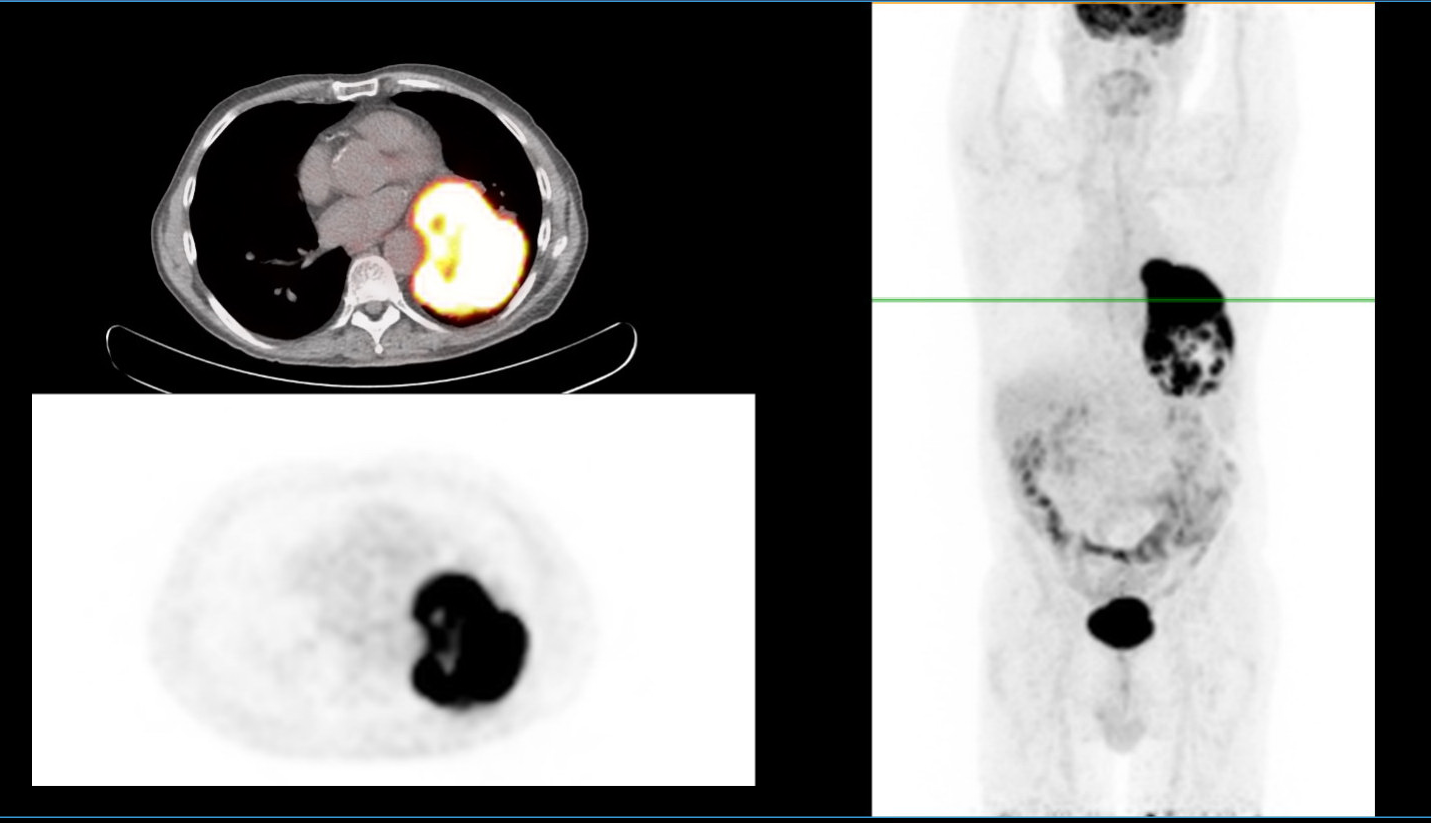
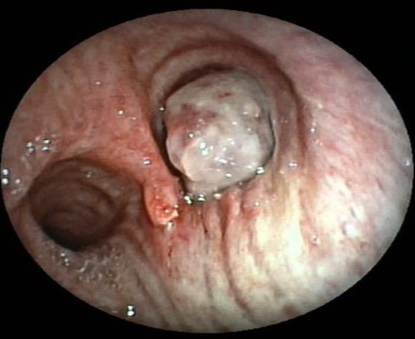
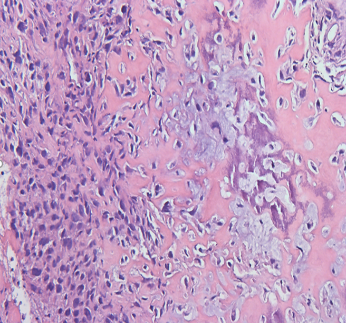
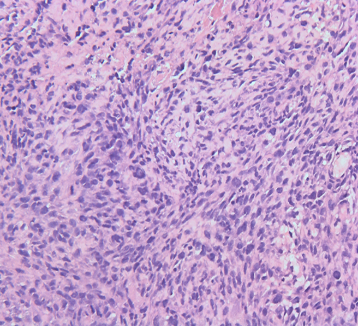
Regarding lesion location, six patients had central lesions (Figures 1a and 1b) and two had peripheral lesions (Figure 1c). A tissue diagnosis was obtained before surgery in seven patients, with the use of bronchoscopy in six patients (Figure 2) and mediastinoscopy in one patient. Only one patient was diagnosed with PCS postoperatively (Table 1). The histopathological picture for all tumors, by definition, was biphasic and composed of an intimate admixture of carcinomatous and sarcomatous elements (Figures 3a and 3b).
Table 1. Characteristics of the patients with PCS tumors |
||||
|
Patient |
Age |
Gender |
Location |
Diameter Radiologic (R) Macroscopic (M) |
|
1 |
50 |
F |
Left upper lobe (central) |
8.5 × 8.2 cm (R) |
|
2 |
65 |
M |
Right upper lobe (central) |
5.5 × 4.5 cm (R) |
|
3 |
76 |
M |
Left upper lobe (central) |
3.6 × 3.5 cm (R) |
|
4 |
72 |
M |
Left lower lobe (peripheral) |
13 × 9 × 6 cm (M) |
|
5 |
70 |
M |
Left lower lobe (peripheral) |
21.5 × 14 × 13.5 cm (M) |
|
6 |
60 |
M |
Right upper lobe (central) |
21 × 18 × 9 cm (M) |
|
7 |
79 |
F |
Right upper lobe (central) |
9.5 × 7 × 7 cm (M) |
|
8 |
64 |
F |
Right upper lobe (central) |
14 × 13 × 3.5 cm (M) |
|
|
|
|
a) |
b) |
|
|
|
|
c) |
|
|
Figure 1. a) Chest CT showing a large endobronchial tumor in the right upper lobe of patient with PCS. b) Chest CT showing right upper lobe collapse with ipsilateral mediastinal shift due to compression/obstruction of right upper lobe bronchus by a central lung mass. c) PET-CT showing a large peripheral tumor in the left lower lobe. |
|
|
|
|
Figure 2. Bronchoscopy showing a large endobronchial tumor obstructing the right upper bronchus. |
|
|
|
|
a) |
b) |
|
Figure 3. Histological images of surgical lung biopsy sample. A mixture of sarcoma and carcinoma components is shown in both pictures (a, b). The biphasic tumor consists of solid sheets of poorly differentiated epithelioid cells, with polymorphic and elongated hyperchromatic nuclei and scattered mitoses, adjacent to which is an abrupt transition to a mesenchymal component, with cartilage and osteoid formation. |
|
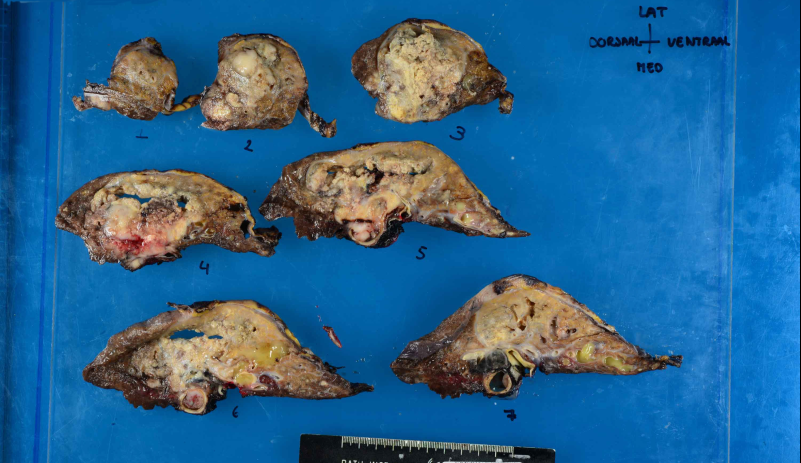
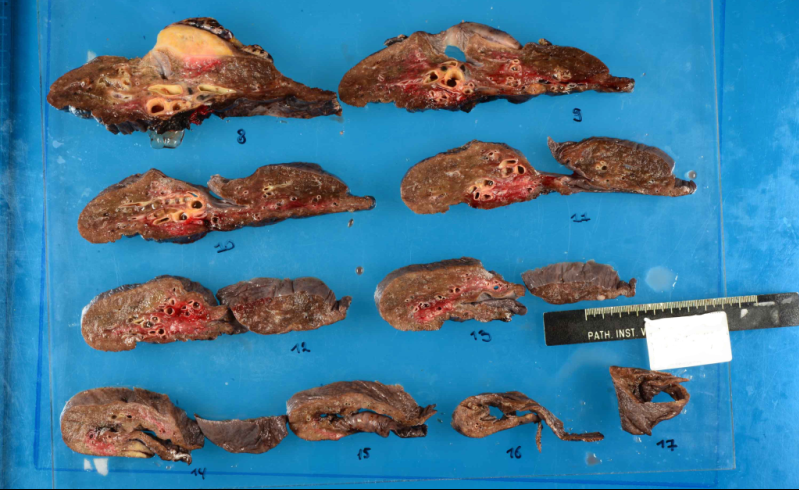
Complete resection was performed in seven patients. This included lobectomy (n = 6) and pneumonectomy (n = 1). Five out of six patients that underwent lobectomy had an upper lobectomy and a lower lobectomy (Table 2). All the patients had a large solid lung tumor whose diameter ranged from 3.5 to 21.5 cm (Figures 4a and 4b).
Table 2. Treatment strategies and follow-up data |
|||||
|
Stage |
Local/ Metastasis |
TNM |
Surgery/ Chemotherapy |
Follow-up |
Outcome |
|
IV |
Metastasis |
T4 N3 M1 |
Chemotherapy |
1 month |
Dead |
|
IB |
Local |
T2A N0 M0 |
Lobectomy |
8 years |
Dead |
|
IB |
Local |
T2A N0 M0 |
Lobectomy |
4 days |
Dead |
|
IIB |
Local |
T3 N0 MO |
Lobectomy |
7 days |
Dead |
|
IIIA |
Local |
T3 N1 MO |
Lobectomy |
6 months |
Dead |
|
IIIA |
Local |
T3 N1 M0 |
Lobectomy, then adjuvant chemotherapy |
3 months |
Dead |
|
IIB |
Local |
T3 N0 MO |
Pneumonectomy |
4 months |
Dead |
|
IIIA |
Local |
T3 N1 M0 |
Neoadjuvant chemotherapy, then lobectomy |
2 years |
Alive |
|
|
|
a) |
|
|
|
b) |
|
Figure 4. Macroscopic images showing a large tumor with an irregular border (a and b). |
Of the patients that underwent complete surgical resection (n = 7), only one was alive at the time of writing. Of the six deceased patients, one survived 8 years, three died in a couple of months due to distant metastasis and cachexia, and two patients suffered postoperative mortality and died in an intensive care unit (ICU).
Chemotherapy is often used in advanced-stage disease including Stages III and IV. Unfortunately, treatment with systemic chemotherapy did not show a significant improvement in PCS patients. One patient with Stage IV PCS died after 2 months of treatment with chemotherapy comprising carboplatin, gemcitabine, and ifosfamide. Two patients received induction chemotherapy for Stage IIIA, one as adjuvant and the other as neoadjuvant chemoradiotherapy using carboplatin and etoposide. Moreover, one patient received radiotherapy as a neoadjuvant, and one patient received immunotherapy.
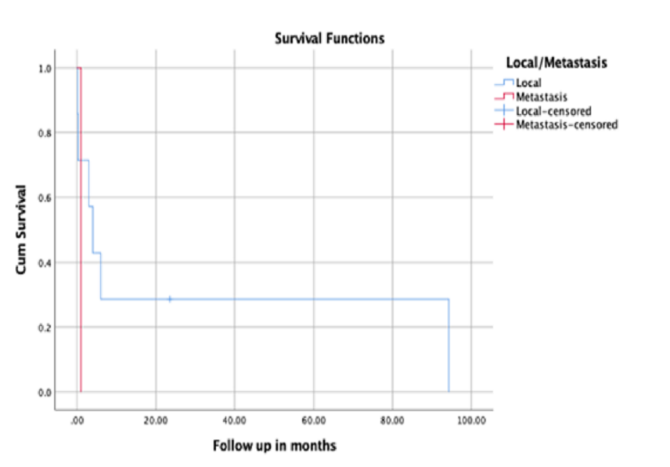
(Figure 5a) shows the survival curve of the patients in regard to the site of the tumor. Localized or metastasized tumors were both associated with a poor prognosis in the patients, with no statistically significant difference between them.
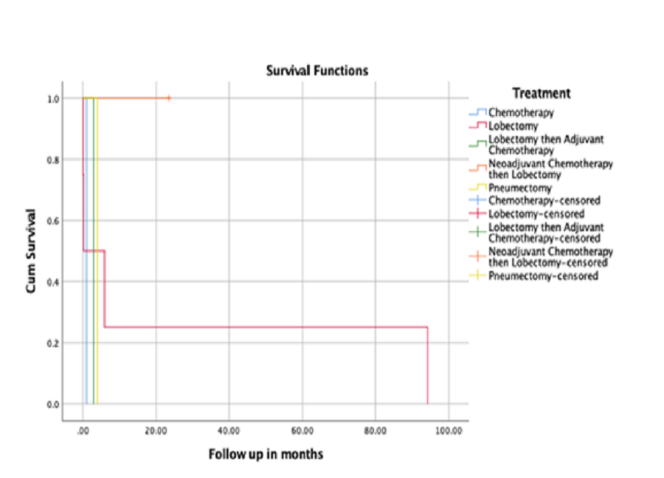
(Figure 5b) shows the survival curve of the patients regarding the treatment received. There was no superior treatment in terms of outcome.
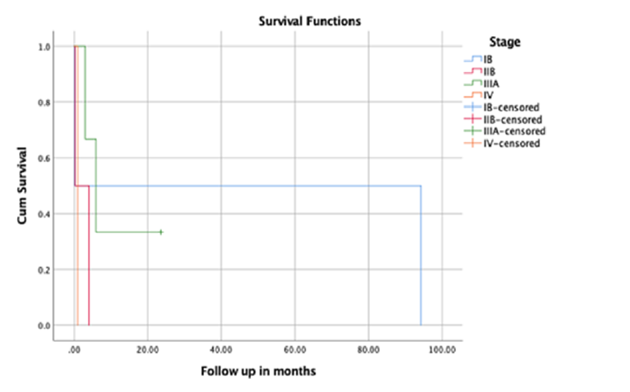
(Figure 5c) shows the survival curve of the patients in regard to the stage of the tumor. No stage had a statistically better outcome.
|
|
|
a) |
|
|
|
b) |
|
|
|
c) |
|
Figure 5. a) Kaplan–Meier survival analysis with follow-up in days with regard to the site. b) Kaplan–Meier survival analysis with follow-up in days with regard to the treatment. c) Kaplan–Meier survival analysis with follow-up in days with regard to the stage. |
PCS is a highly malignant and biphasic tumor,[1] consisting of a mixture of non-small cell lung carcinoma and sarcoma-containing heterologous elements,[4] with a reported incidence of 0.1%–0.3 % of all lung malignancies.[2, 3]
It is usually a large tumor (>5 cm), some lesions being as large as 21 cm or more, and has a high tendency to invade adjacent structures such as the pleura, chest wall, diaphragm, or mediastinum.[23] In the current study, the tumor diameter was 3.5–21.5 cm. Further, the study patients were aged 50–79 years and predominantly male (5/8). Additionally, all patients were smokers. Prior research shows that PCS strongly affects heavy smokers, and some reports describe asbestosis.[24]
Carcinosarcoma has been reported in most organs where primary carcinoma can occur, including the uterus, breast, thyroid gland, esophagus, and lung.[25] The epithelial component is defined by the presence of a typical carcinoma, usually squamous cell carcinoma or adenocarcinoma, while the sarcomatous element can consist of rhabdomyosarcoma, osteosarcoma, or chondrosarcoma.[3, 4, 26] It is now accepted that both components derive from a typical stem cell, in which a carcinoma undergoes sarcomatoid changes.[27, 28] The proposed pathogenesis of carcinosarcoma includes (a) malignant transformation of hamartoma, (b) simultaneous malignant transformation of epithelial elements and stromal components, (c) malignant transformation of cancer-derived stroma, (d) sarcomatous changes of carcinoma, and (e) carcinomatous changes of sarcoma.[29] The carcinoma and sarcoma elements can usually be identified histologically, but immunohistochemistry can be helpful in less differentiated cases. Squamous cell carcinoma is positive for p63 and p40, and adenocarcinoma is positive for TTF-1 and keratin 7. The sarcomatous elements also mimic their counterparts in other organs, as rhabdomyosarcoma shows immunoreactivity with desmin and myogenin, and chondrosarcoma with S100.[4, 30] The most frequent epithelial component was squamous cell carcinoma (46%), followed by adenocarcinoma (31%) and adenosquamous carcinoma (19%), whereas sarcomatous elements most frequently included rhabdomyosarcoma, chondrosarcoma, osteosarcoma, or combinations of these elements.[31] Takeda et al. reported squamous cell carcinoma as the most common epithelial component.
PCS presents in two locations: central endobronchial and peripheral. Koss et al. reported an extensive study for PCS of 66 patients and described that 62% of patients had central and 38% peripheral lesions. Conversely, Sökücü et al. reported a retrospective study of six patients with PCS; four had peripheral tumors and two had central tumors,[32] and Yazıcı et al. reported a peripheral location in 85.7%. In our retrospective study of eight patients with PCS, six had a central endobronchial lesion and two had a peripheral lesion.
The most common presenting complaint of the study patients was a cough with dyspnea. The clinical presentation depends on the location of the tumor. Patients with the peripheral type typically present with a cough, dyspnea, and hemoptysis, similar to other endobronchial tumors. Meanwhile, the peripheral type is often asymptomatic in the early stages, and symptoms appear with the involvement of adjacent organs or structures such as the mediastinum, pleura, and thoracic wall.[32] In addition, PCS can be associated with paraneoplastic syndromes. These are not explicitly described but may manifest as systemic, skin, kidney, endocrine, hematological, or neurological affectations.[33]
Many previous reports considered it challenging to diagnose PCS preoperatively because the composition of the different histopathological structures means that the biopsy sample taken often reflects one element of the tumor, mainly when centrally located. In addition, peripheral tumors are difficult to reach by bronchoscopy and many are diagnosed on postoperative pathological analysis.[19, 32] In contrast, in our study, seven out of eight patients were diagnosed preoperatively, with the use of bronchoscopy in six patients and mediastinoscopy in one patient.
Metastasis is frequent in PCS, and the most common sites for metastasis are the lymph nodes, followed by the kidneys, bones, liver, and brain.[31] In our study, three patients were found to have metastasis: two had distant metastasis and one had metastasis in the pleura. Prior studies showed that metastatic lesions were carcinomatous (50%) or sarcomatous (40%) and that only 10% had both components.[19]
The primary treatment of PCS in the early stages is surgical resection, in addition to standard adjuvant chemotherapy for high-risk Stages IB, II, and IIIA. Palliative chemotherapy may be used in advanced-stage patients.
Poor responses to chemotherapy have been demonstrated in past studies.[22] Liang et al. reported in 33 patients that chemotherapeutic regimens, including platinum-based combinations and doxorubicin- or ifosfamide-based combinations, failed to improve patient survival.[2] Caviglia et al. reported poor sensibility of chemotherapy. Ito et al. reported that five patients received palliative chemotherapy and demonstrated no clinical benefits. Langer et al. reported a case that received six cycles of chemotherapy with cisplatin and doxorubicin, which resulted in partial remission. Elalami et al. reported that a patient with advanced PCS, which was Stage IV, received palliative chemotherapy with cisplatin and docetaxel without effect, and the patient died 3 months after diagnosis.[34] Sakane et al. described a partial effect of chemotherapy as adjuvant therapy after complete resection for a patient with blastomatoid PCS.[35] In our study, three patients received chemotherapy. One patient with Stage IV PCS received palliative chemotherapy with carboplatin, gemcitabine, and ifosfamide for four cycles. The patient did not respond and died 1 month after treatment. The other two patients received chemotherapy as induction for Stage IIIA PCS. One received two cycles of chemotherapeutic agents, cisplatin, docetaxel, and then nivolumab, but with no response, and died 3 months after treatment. The other received induction neoadjuvant chemoradiotherapy with four cycles of chemotherapeutic agents, carboplatin, and etoposide. The patient showed partial response and underwent a right upper lobectomy, and was alive at the time of writing.
Alternative therapeutic approaches have been proposed. Zhang et al. reported that patients with PCS with positive expression for PD-L1 obtained a significant benefit from nivolumab treatment.[36] Further, the role of molecular targeted therapy, such as the EGFR, K-RAS pathway, and echinoderm microtubule-associated protein ALK, warrants further research.[22]
Regarding prognosis, the median survival time was reported as 9–12 months after potentially curative surgical resection,[26, 37] and fewer than 10% of patients were thought to survive 2 years. In our study, complete resection was performed in seven patients, of which only one was alive at the time of writing. According to the literature, factors that adversely affect the prognosis and survival time include the size of the tumor and lymph node involvement.
The limitations of the current study include the fact that the sample size was small; this is because this type of cancer is very rare and a limited number of patients were enrolled during the study period at AUMC-VUMC. Future studies, preferably multicenter studies, should consider increasing the sample size.
PCS is a sporadic cancer with an aggressive nature and poor prognosis. According to the literature, the survival time of PCS does not exceed that of other pulmonary cancers, even after complete surgical resection, which is considered an effective treatment. There is no clear evidence that chemotherapy prolongs survival, and most reports have indicated that advanced PCS responds poorly to chemotherapy.
Grateful acknowledgments are made to the Department of Pulmonology and Pathology Division at Amsterdam University Medical Center AUMC-VUMC, Amsterdam, The Netherlands.
None.
None.
None.
|
||||||||