|
|
|
|
Prevalence, Types, and Management of Maxillary Sinus Carcinoma: A Systematic Review
Malik Azhar Hussain1*, Taif Khalaf Alanazi2, Renad Lafi Alanazi2, Jawaher Awad Alshammari2, Amwaj Nawaf Alshammari2, Najd Turki M Alanazi2
1Department of General Surgery, Faculty of Medicine, Northern Border University, Arar, Saudi Arabia. 2Faculty of Medicine, Northern Border University, Arar, Saudi Arabia.
Abstract
As Maxillary Sinus Carcinoma (MSC) is a rare and serious condition and due to the variable treatment modalities, that are seeking to manage it, this systematic review is to assess the prevalence, types, and effectiveness of Chemoradiotherapy (CRT) and Proton Therapy (PBT) in the management of MSC. PubMed, Web of Science, Science Direct, EBSCO, SCOPUS, Wiley, and Cochrane Library were searched. Study articles were screened by title and abstract using Rayyan QCRI then a full-text assessment was implemented. A total of twelve studies with 468 patients and 335 males were included. MSC was prevalent in Japan and SCC was the most common histopathological type of MSC, followed by adenoid cystic carcinoma. PBT is an effective therapeutic modality in managing MSC and offers a promising future in the treatment of head and neck cancer. Proton beam therapy's precise function will become clearer as it becomes more widely used and as clinical research's purview broadens. IMRT and CRT have high survival rates, good local control, and a low risk of recurrence. MSC was prevalent in Japan and SCC was the most common histopathological type of MSC.
Keywords: Maxillary sinus carcinoma, Chemoradiotherapy, Proton therapy, Systematic review
Only 0.1% of all cancers and 1% of all malignant head and neck tumors are maxillary sinus malignant tumors, making them extremely uncommon.[1, 2] The incidence is roughly 0.5-1/100.000 per year.[3] Men over 50 years old have the highest prevalence.[3] Squamous cell carcinoma (SCC) is the histological diagnosis for 30–50% of sinonasal malignancies, and the maxillary sinus accounts for 26-47% of these cases.[2, 4, 5] Although diagnostic and treatment methods have made significant strides, 5-year survival rates are still dismal and range from 34 to 49%.[6-8]
The advanced stage of the disease is one of the most significant indicators of a poor prognosis. Maxillary sinus tumors are frequently discovered after they have already grown significantly or invaded nearby structures, causing catastrophic malfunctions such as diplopia.[9, 10] This is because they grow in air-filled spaces and provide vague symptoms until they reach a sizeable volume. MSC is incidentally discovered in 12% of cases because the patients have no symptoms.[11] Another significant factor in delayed diagnosis is the maxillary sinus's inability to be directly examined and palpated, as opposed to the oral cavity.[12]
The local expansion of 70–80% of MSC is categorized as T3 or T4 at the time of diagnosis.[4] A locally progressed tumor lowers the patients' prognosis, according to several studies.[13] T-classification, regional and distant metastasis (N- and M-classification), invasion of nearby tissues such as the orbit and skull base, age, as well as the types and sequences of treatment are significant prognostic markers for MSC.[9, 14] For locally advanced laryngeal and pharyngeal SCC, chemotherapy (CRT) is the preferred treatment. However, CRT does not always result in excellent treatment outcomes for patients with MSC.[15]
For patients with head and neck cancer, PBT has shown promising results in terms of disease management and treatment outcomes while preserving a good quality of life. Although proton therapy has been used therapeutically to treat cancer for many years, its use has been constrained because of its high cost and scarcity. Proton therapy is now more widely used and more reasonably priced thanks to technological developments and improvements in medical equipment.[16]
The radiation oncologist faces a challenging task while treating paranasal sinus cancers because these tumors are anatomically located close to numerous vital normal tissues, including the brain, optic nerves, eyes, optic chiasm, brainstem, spinal cord, parotid glands, and lacrimal glands. High-dose radiotherapy, which is frequently given together with chemotherapy, may cause severe normal tissue harm.[17]
This systematic review was conducted following accepted standards (Preferred Reporting Items for Systematic Reviews and Meta-Analyses, PRISMA).
This was a systematic Review.
From November to December 2022.
The purpose of this systematic review is to assess the effectiveness of CRT and PBT in the management of MSC.
To locate the pertinent literature, a thorough search of five main databases, including PubMed, Web of Science, Science Direct, EBSCO, Scopus, Wiley, and Cochrane Library, was carried out. We limited our search to English and took into account each database's specific needs. The subsequent keywords were transformed into Mesh terms in PubMed and utilized to locate the relevant studies; "Maxillary sinus carcinoma," "MSC," "Maxillary sinus cancer," "Maxillary sinus tumor," "Maxillary sinus neoplasm," "Radiotherapy," "Chemotherapy," "Chemoradiotherapy," "Proton therapy," "Treatment," and "Management." The necessary keywords were matched using the Boolean operators "OR" and "AND." The search results included full-text English-language publications, openly downloadable articles, and human trials.
According to the research's standards, the following criteria had to be met for the subjects to be included: male or female patients with MSC who underwent therapeutical trials, including RCT and BPT.
All subsequent publications, ongoing investigations, and assessments of completed studies that did not focus on one of these subjects were excluded. Despite the rarity of this condition, we did not include case reports.
We used Rayyan (QCRI) to search for duplicates in the search strategy's output.[18] The relevance of the titles and abstracts was determined by the researchers by reducing the combined search results based on a set of inclusion/exclusion criteria. The reviewers read every word of the papers that satisfied the requirements for inclusion. The writers addressed dispute-resolution techniques. Using a made-up data extraction form, the approved study was uploaded. The authors extracted data about the study titles, authors, study year, study designs, country, population type, participant number, mean age, gender, histological types, used therapy, and main outcomes.
Summary tables compiled from the information gathered from the eligible studies were produced to provide a qualitative summary of the included study components and outcomes. The optimal way to use the data from the included study articles was selected after data extraction for the systematic review. Studies that met the full-text inclusion criteria but did not provide data on CRT or PBT used in MSC patients were excluded.
Using the ROBINS-I risk of bias assessment approach for non-randomized trials of therapies, the quality of the included studies was assessed.[19] Confounding and participant selection for the study, classification of interventions, deviations from intended interventions, missing data, assessment of outcomes, and choice of the reported result were the seven issues that were examined.
Results and Discussion
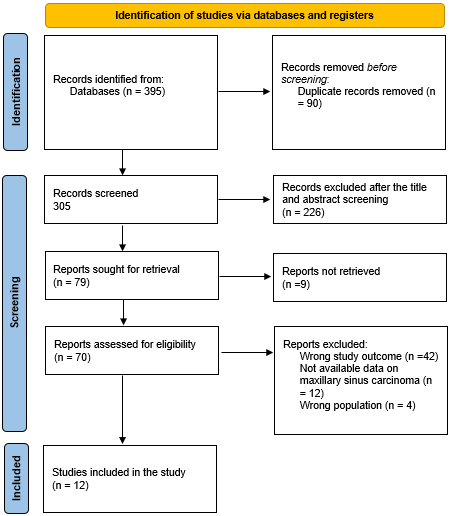
A total of 395 study articles resulted from the systematic search, and then 90 duplicates were deleted. Title and abstract screening were conducted on 305 studies, and 226 studies were excluded. 79 reports were sought for retrieval, and only 9 articles were not retrieved. Finally, 70 studies were screened for full-text assessment; 42 were excluded for wrong study outcomes, 12 for unavailable data on therapeutical approaches for MSC, and 4 for the wrong population type. Twelve eligible study articles were included in this systematic review. A summary of the study selection process is presented in Figure 1.
|
|
|
Figure 1. PRISMA flowchart summarizes the study selection process. |
Table 1 includes the sociodemographic characteristics. A total of twelve studies with 468 MSC patients and 335 males were included. Ten studies were conducted in Japan,[20-29] one in India,[30] and one in South Korea.[31] Their age ranged from 18 to 87 years. The most common histopathological types were SCC and adenoid cystic carcinoma.
Table 1. Sociodemographic characteristics of the included participants |
||||||
|
Study |
Country |
Population type |
Participants (n) |
Age range |
Males (%) |
Histopathological type |
|
Sugiyama et al. 2019[20] |
Japan |
Patients with MSC |
26 |
25-83 |
21 (81%) |
SCC (92%), spindle cell carcinoma (4%), and small cell carcinoma (4%) |
|
Narita et al. 2021[21] |
Japan |
Patients with MSC |
15 |
26-85 |
10 (66.7) |
SCC |
|
Nakamura et al. 2016[22] |
Japan |
Patients with MSC |
26 |
25-79 |
19 (73.1) |
SCC (57.9%), adenoid cystic carcinoma (23.1%), spindle cell carcinoma (7.7%), adenocarcinoma (3.8%), melanoma (3.8%), and neuroendocrine carcinoma (3.8%) |
|
Narita et al. 2019[23] |
Japan |
Patients with advanced-stage MSC |
20 |
18-75 |
13 (65) |
SCC |
|
Nandwana et al. 2018[30] |
India |
Patients of advanced-stage MSC |
25 |
61 ± 9 (mean) |
16 (64) |
SCC |
|
Heianna et al. 2022[24] |
Japan |
Patients of T4 MSC |
22 |
36-86 |
20 (91) |
SCC |
|
Nishino et al. 2000[25] |
Japan |
Patients with MSC |
78 |
38-87 |
48 (61.5) |
SCC (80.8%), adenoid cystic carcinoma (2.6%), mucoepidermoid carcinoma (2.6%), rhabdomyosarcoma (2.6%), adenocarcinoma (2.6%), acinic cell carcinoma (1.3%) Carcinosarcoma (1.3%), malignant melanoma (1.3%), and malignant mixed tumor (1.3%). |
|
Konishi et al. 2020[26] |
Japan |
Patients with locally advanced MSC |
54 |
38-76 |
45 (83.3) |
SCC (98.1%) and undifferentiated carcinoma (1.9%) |
|
Makino et al. 2020[27] |
Japan |
Patients with MSC |
19 |
35-74 |
14 (73.7) |
SCC |
|
Homma et al. 2013[28] |
Japan |
Patients with MSC |
54 |
29-73 |
43 (79.6) |
SCC |
|
Suh et al. 2016[31] |
South Korea |
Patients with MSC |
19 |
26-84 |
7 (37) |
SCC (51%), adenoid cystic carcinoma (29%), sarcoma (6%), and others (14%) |
|
Yoshimura et al. 2002[29] |
Japan |
Patients with MSC |
110 |
25-83 |
79 (71.8) |
SCC |
Table 2. Characteristics and outcomes of the included studies. |
|||||
|
Study |
Study design |
Objectives |
Type of Therapy |
Key findings |
ROBIN-I |
|
Sugiyama et al. 2019[20] |
Comparative study |
Effect of PBT on the normal tissue as a treatment for MSC |
PBT |
The dose to the ipsilateral optic nerve is decreased during intensity-modulated PBT when a multi-leaf collimator (MLC) is used to treat MSC. |
High |
|
Narita et al. 2021[21] |
Cohort study |
To look at the dosimetric effects of PBT-induced anatomical changes in MSC |
PBT |
After the start of the treatment, the tumor shrank by about 3–4 weeks. OARs received a higher dosage as a result. It is advised to confirm the state of the tumor and to improve the dose distribution in the latter part of the treatment course to address the degradation of the dose distribution brought on by these changes during radiotherapy. |
Moderate |
|
Nakamura et al. 2016[22] |
Cohort study |
The effectiveness and side effects of treating MSC with a combination of PBT and intra-arterial infusion of cisplatin through the superficial temporal artery |
PBT |
Most patients who get PBT and chemotherapy for MSC with intra-arterial infusion via a superficial temporal artery will have their organs preserved and cured. In the current trial, drug-related toxicities were generally under control. |
Moderate |
|
Narita et al. 2019[23] |
Comparative study |
The impact of anatomical change on the passive scattering PBT dose distribution for MSC |
PBT |
Even after accounting for the impact of anatomical change, PBT was found to be more effective. As a result, it is anticipated that reliable contralateral vision preservation will be possible while receiving the best target coverage. |
Moderate |
|
Nandwana et al. 2018[30] |
Retrospective study |
To investigate the effects of survival in patients who underwent postoperative radiation for advanced-stage MSC. |
IMRT |
Moderate |
|
|
Heianna et al. 2022[24] |
Retrospective study |
To assess the effectiveness and safety of intra-arterial chemotherapy and radiation therapy for T4 MSC. |
CRT |
The patients with locally progressed MSC may benefit from intra-arterial chemoradiotherapy with docetaxel and nedaplatin for loco-regional control and survival. |
High |
|
Nishino et al. 2000[25] |
Retrospective study |
To evaluate the outcomes of our combined therapy for treating patients with MSC, including perioperative irradiation, regional chemotherapy, and conservative surgery. |
CRT |
Control of the primary tumor location is crucial. Combining therapy with conservative surgery, radiation, and local chemotherapy appears to be efficient for local control and maintenance of ocular function. |
Moderate |
|
Konishi et al. 2020[26] |
Retrospective study |
To treat locally advanced MSC with radiotherapy and concurrent super-selective RADPLAT |
CRT |
Patients who received 70 Gy of IMRT had excellent local control rates without experiencing an increase in side events. |
Moderate |
|
Makino et al. 2020[27] |
Retrospective study |
To look at the pathological evaluations after RADPLAT for MSC therapy outcomes |
CRT |
In addition to having a minimal risk of adverse effects, pathological analysis suggests that RADPLAT might be a useful therapy for treating locally progressed MSC. Increasing the RADPLAT treatment intensity might be a good alternative to more invasive surgery. |
High |
|
Homma et al. 2013[28] |
NA |
The effect of RADPLAT on MSC therapy outcomes |
CRT |
Patients with SCC-MS treated with RADPLAT had good local progression-free survival rates and appropriate acute and late toxicity rates. |
Moderate |
|
Suh et al. 2016[31] |
Retrospective study |
Treatment outcomes of IMR for maxillary sinus carcinoma |
IMRT |
In patients with MSC, postoperative IMRT produced excellent disease control and ought to be the first course of treatment. |
Moderate |
|
Yoshimura et al. 2002[29] |
Retrospective study |
To assess the efficacy of trimodal combination therapy to treat primary MSC using radiation, intra-arterial chemotherapy, and antrotomy. |
CRT |
The T stage of the tumor determines the overall result; however, trimodal combination therapy offers good local control. |
Moderate |
To the best of our knowledge, this is the first systematic review to emphasize the published literature on PBT and CRT as management modalities for patients with MSC. However, this systematic review is limited by the lack of quantitative assessments of survival rates and tumor control on using these therapeutic options. Our study is also limited by the lack of earlier longitudinal, cohort, and pooled analyses for the management of MSC.
We noted that most of the included studies (10 out of 12 studies) were conducted in Japan. This is documented in some cancer registries that in comparison to international statistics, the cancer of the nasal sinus has a comparatively high incidence in Japan. In Asia, MSC occurs more frequently than in Western nations.[32, 33]
We also documented that the most common histopathological types of MSC were SCC and adenoid cystic carcinoma. This was consistent with the previous investigation.[33] Malignancies of the nasal and paranasal cavities have a wider range of histological categories than those of the larynx and pharynx; however, squamous cell carcinoma is the most common kind. This is due to the ciliated pseudostratified columnar epithelium that makes up the mucosa of the nasal and paranasal canals, which evolves into squamous epithelium where cancer originates. Because squamous cell carcinoma responds to CRT reasonably well, multimodal therapy is used.[34]
PBT was effective in managing MSC and its impact on the anatomical changes in this study. Narita et al. reported that the tumor shrank by about 3–4 weeks of PBT and the organs at risk (OARs) received a higher dosage as a result.[21] Historically, oropharyngeal cancer has been successfully treated with IMRT, which has fewer side effects (such as xerostomia). To provide the highest possible standard of living, treatment-related toxicities must be further decreased as the percentage of young, HPV-positive patients rises. Proton therapy has the advantage of sparing contralateral oropharyngeal and nasopharyngeal tissue from radiation, whereas IMRT frequently causes unneeded radiation of healthy tissue because of the nature of the photon. Particularly following a transoral robotic surgery, proton treatment can be used to lessen incidental radiation administered outside of the target volume.[35]
The use of proton radiation treatment for head and neck cancer appears to be promising at this time. Proton radiation therapy is becoming more popular, and as a result, more clinical studies and technological developments will shed light on its genuine usefulness as a therapeutic choice for the treatment of head and neck cancer. Additionally, stronger treatment plans and quality assurance systems will be created with the aid of automated proton plan adaption and advance in proton delivery to precisely deliver the radiation dosage to the required target volumes.[36]
We also reported that IMRT and CRT have high survival rates, good local control, and a low risk of recurrence. With a 6.5% increase in survival at five years, concurrent CRT appears to be more effective than sequential methods. The outcomes of using radiotherapy and chemotherapy in order were poorer.[37] The best time to administer CRT—preoperatively or postoperatively—remains up for debate. The effectiveness and safety of neoadjuvant CRT followed by radical surgery in treating oral squamous cell carcinoma have been demonstrated in numerous trials.[38, 39]
Recent research by our team has shown that in patients with oral squamous cell carcinoma and stage N2 cervical lymph node involvement, neoadjuvant CRT is preferable to primary surgery, followed by adjuvant CRT.[30] Preoperative CRT facilitates full resection, lowers the likelihood of perioperative tumor cell spread with implanted metastases, and provides the chance for tissue preservation and retained functional integrity. Due to better oxygenation of the tumor, the radiotherapeutic impact is enhanced in contrast to postoperative CRT.[40] However, this method of treatment may be linked to a higher incidence of pre-and postoperative problems.
PBT is an effective therapeutic modality in managing MSC and offers a promising future in the treatment of head and neck cancer. Proton beam therapy's precise function will become clearer as it becomes more widely used and as clinical research's purview broadens. IMRT and CRT have high survival rates, good local control, and a low risk of recurrence. MSC was prevalent in Japan and SCC was the most common histopathological type of MSC.
Many thanks to Dr. Malik Azhar Hussain; Consultant of General Surgery, Faculty of Medicine, Northern Border University, Arar, Saudi Arabia, for his continuous help, support, and encouragement to complete this work.
None.
None.
None.
|
||||||||