Deniz Publication
Clinical Cancer Investigation Journal
ISSN Print: 2278-1668, Online: 2278-0513
ISSN Print: 2278-1668, Online: 2278-0513
Oral Cancer Staging and Clinicopathologic Features Presenting to Oral & Maxillofacial Surgery Practice in Saudi Arabia
Basem T. Jamal1,2*
1Consultant and Associate Professor Oral & Maxillofacial Surgery/Head and Neck Surgical Oncology, King AbdulAziz University, Jeddah, Saudi Arabia. 2Affiliate Consultant, Oral & Maxillofacial Surgery Department, King Abdullah Medical City, Makkah, Saudi Arabia.
Abstract
The most common type of head and neck cancer, oral cancer (OC), is the 16th most common malignancy and the 15th most frequent cause of cancer-related deaths in the world. There has been an increase in the incidence of OC in Saudi Arabia in recent years. The survival rate of oral cancer is one of the lowest in the world and still, unfortunately, a large number of OC cases are discovered in advanced stages. The purpose of this study is to assess the prevalence of advanced stages of oral cancer in maxillofacial surgical oncology practice in Saudi Arabia. Patients diagnosed with oral cancer presented to the oral and maxillofacial surgery clinic at 2 institutions where the author's work was identified. Primary data extracted from the database included age, sex, histologic subtype, tumor site, and TNM stage. A total of 156 records of patients with oral cancer confirmed by histopathology were assessed. The mean age of patients was 59.2 years. The majority of the patient presented at an advanced stage, 79% with a distribution as follows: 11% Stage I, 10% Stage II, 16% Stage II, and 63% Stage IV. The positive nodal disease was diagnosed in 58% of the tumors. The study reflects the high prevalence of advanced oral cancer cases in Saudi Arabia as experienced by an oral and maxillofacial surgery practice and it highlights the need for more collaboration between the centers to ensure timely diagnosis and referral of oral cancer patients.
Keywords: Oral cancer, Advanced cases, Saudi Arabia, Maxillofacial surgery
The most common type of head and neck cancer, oral cancer (OC), is the 16th most common malignancy and the 15th most frequent cause of cancer-related deaths in the world.[1] The geographical incidence of this cancer is, however, extremely variable, and several factors are involved, including cultural habits, availability of health services, and economic circumstances.[2] It is estimated that there were 377,713 new cases of lip and oral cancer worldwide in 2020 and that there were 177,757 deaths due to this disease.[3] Globally, over 450,000 patients are diagnosed with OC each year, and the five-year survival rate is below 50%.[4, 5]
In Arab Gulf countries, oral cancer is relatively uncommon; however, Saudi Arabia is an exception to this rule.[6] There has been an increase in the incidence of OC in Saudi Arabia in recent years. The Tumor Registry of King Faisal Specialist Hospital & Research Center in Riyadh indicates that OC accounts for 4% of all cancers in Saudi Arabia. They found that OC was the fifth most common cancer among males and the eleventh most common cancer among females. Oral cancer is more prevalent in Saudi Arabia than in surrounding Gulf countries, such as Kuwait and the United Arab Emirates, which share similar geographical and cultural characteristics.[7] Approximately 26 percent of all head and neck cancers detected annually in KSA are oral cancers, most of which are in advanced stages requiring palliative care.[8] Several studies have shown that the use of Shamma, a form of smokeless tobacco, is associated with the high incidence of oral cancer mentioned earlier.[7, 9]
The survival rate of oral cancer is one of the lowest in the world. Despite the ease with which malignant lesions may be detected in the oral cavity, it is unfortunate that a significant number of oral cancer cases are discovered at an advanced stage. According to a meta-analysis, diagnosis delay was likely to be a contributing factor to advanced-stage OC and mortality.[7, 10]
The survival rate for oral squamous cell carcinoma has only marginally improved despite advancements in imaging
techniques (including computed tomography, positron emission tomography, magnetic resonance imaging, and ultrasound), surgical techniques, radiation therapy sources and delivery methods, and combination with chemotherapy.[11, 12] Many patients who have had successful treatment for oral cancer may experience functional and cosmetic impairments, including difficulties eating, swallowing, speaking, and disfigurement which may have a significant adverse impact on their quality of life.[13] Early detection of oral cancer is the most effective way to reduce morbidity and disfigurement as well as improve survival rates.[14] Worldwide statistics on oral cancer staging prevalence show that 55-75% of oral cancer patients are diagnosed at advanced stages (stages III–IV), with corresponding 5-year overall survival ranging from 33-63%.[1, 11, 15-26] A systematic review of oral cancer in Saudi Arabia found that all patients enrolled in the study visited the hospital at an advanced stage, and the 5-year survival rate varied from 12.9% to 24.4%.[27]
In general, early detection of oral cancer improves survival rates to more than 80%, compared to less than 20% for advanced diseases worldwide.[28] The purpose of this study is to assess the prevalence of advanced stages of oral cancer in maxillofacial surgical oncology practice in Saudi Arabia.
Materials and Methods
Patients diagnosed with oral cancer presented to the oral and maxillofacial surgery clinic at 2 institutions where the author's work was identified. The institutions are King Abdulaziz University Hospital and King Abdullah Medical City, Saudi Arabia. Records from 2015-2022 of patients treated at the oral and maxillofacial surgery department were included.
Primary data extracted from the database included age, sex, histologic subtype, tumor site, and TNM stage. The primary focus of this study is to report on the prevalence of advanced-stage oral squamous cell carcinoma in Saudi Arabia as experienced in maxillofacial oncology practice.
Tumors of salivary glands origin, melanomas, sarcomas, as well as verrucous carcinomas were excluded. 156 records of patients with oral cancer confirmed by histopathology were reviewed. Patients were categorized as early (I & II) or advanced (III & IV) stages and staging was assessed using the American Joint Committee on Cancer TNM staging system eighth edition. Age was analyzed as a continuous variable. We obtained information regarding the patient's age, gender, anatomical location, and histopathological diagnosis for every case. Lesions were categorized according to the site as lip, tongue, the floor of the mouth (FOM), cheek (buccal mucosa), mandible, retromolar area, and maxilla (palate).
Results and Discussion
A total of 156 patients had histologically diagnosed squamous cell carcinoma of the oral and maxillofacial area. Of these cases, 55% were men and 45% were women. The mean age of patients was 59.2 years (S.D. = 15.2), (range, 21–93 years). The median age was 60.5.
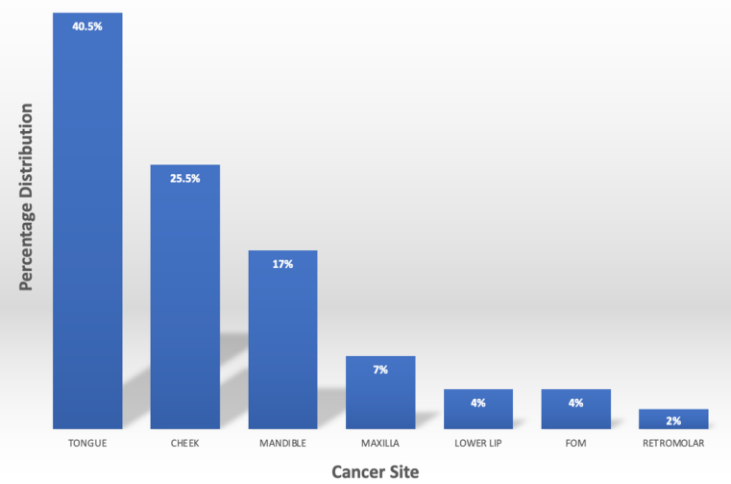
The percentage distribution of the affected areas was: 40.5% tongue, 25.5% cheek, 17% mandible, 7% maxilla, 4% lower lip, and FOM, and finally 2% retromolar area. The frequency of distribution among the oral anatomical sites is shown in Figure 1.
|
|
|
Figure 1. Frequency of distribution among the oral anatomical sites |
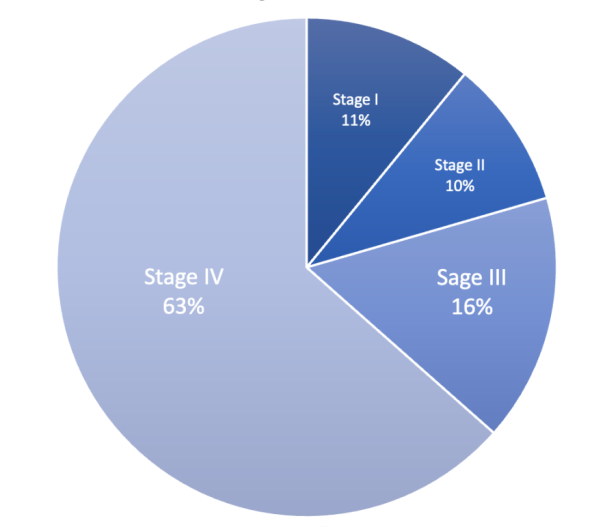
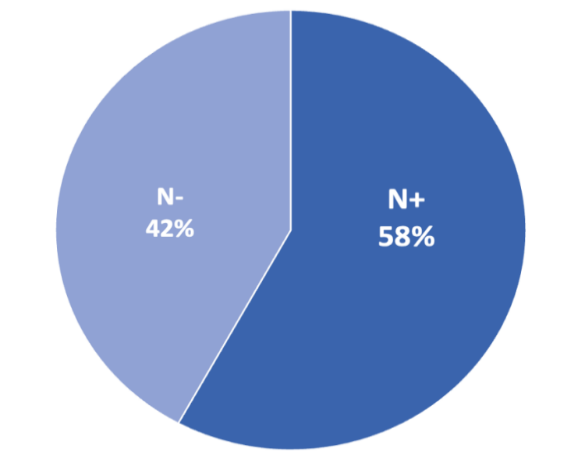
The majority of the patient presented at an advanced stage, 79% with a distribution as follows: 11% Stage I, 10% Stage II, 16% Stage II, and 63% Stage IV as shown in Figure 2. The positive nodal disease was diagnosed in 58% of the tumors, the majority of which with extranodal extension (ENE). Figure 3 shows the prevalence of the positive nodal disease.
|
|
|
Figure 2. Oral Cancer staging |
Over three-quarters of the study, the cohort had advanced oral cancer, and the majority of them were male. Cancer patients with advanced stages were found to be older than those with early-stage cancers.
|
|
|
Figure 3. Nodal disease among the cohort of patients |
Oral cancer remains associated with a poor prognosis despite improvements in diagnosis and treatment; in large part due to a delay in the diagnosis of the disease until it is at a late stage. A study of the national cancer database in the USA between 1998 to 2006 revealed that late-stage disease ranged from 32.5-36%[29] Another study on oral cancer patients in Memorial Sloan Kettering Cancer Center from 1985-2015 of a cohort of over 2000 patients revealed advanced-stage cancer in only 25% and hence the 5-year overall survival of 64.4%.[12] However, that overall survival was not the same across the US with the SEER database indicating 5-year survival ranging from 42.7-52%.[30]
It has been recognized that the stage of the disease at diagnosis is one of the most significant prognostic factors in oral cancer. When oral cancer is detected in an early stage when it is amenable to single modality therapy, there is the best chance of reducing mortality from these diseases in the short term. Unfortunately, two-thirds of patients with oral cancer are still diagnosed at an advanced stage of the disease (stage III and IV) [31, 32] having a 5-year survival rate of 50% or less.[33] As opposed to approximately 80% survival rate in patients with localized disease, which makes the differences in mortality rates based on staging very apparent.[34] In Brazil, Kowalski et al. have demonstrated the potential for clinical upstaging of head and neck cancer before treatment initiation. They also demonstrated that the median 5-year survival rate of patients with clinical upstaging before treatment which was 17.2 months was significantly lower than patients without clinical upstaging and who received treatment within 1-3 weeks and they had a 5-year survival rate of 32.7 months.[35] According to Tsai et al. patients with oral cancer in Taiwan who were treated after 30 days from diagnosis had a lower overall survival rate than those who were treated within 30 days; the trend observed remained unchanged after stratification by the initial stage of the tumor at diagnosis.[36] Van Harten et al. found that longer waiting times for treatment initiation were significantly associated with poorer overall survival in patients with head and neck cancer in the Netherlands.[37]
Our study findings reflect a staggering nearly 80% prevalence of advanced oral cancer cases most of which are in stage 4, 63%. A subset analysis of the patient following the COVID pandemic starting from March 2020 at one of the centers reviewed in the study shows an advanced stages prevalence of 88%. This high incidence of advanced cases is also manifested in the high prevalence of positive nodal disease which occurred in 58% of the cases compared to 29% of the cohort of the patient from Memorial Sloan Kettering Cancer Center.[12] Throughout Saudi Arabia, the prevalence of oral cancer varies by region, with a 30-fold difference in age-standardized rates between the lowest and highest incidences. For instance, Jazan (Gizan) ranked highest in head and neck cancer prevalence in Saudi Arabia; more specifically, oral cancer ranked first among females and second among males.[38] In several studies, the cause of the high incidence of oral cancer in the Jazan region has been investigated.[9, 39, 40] These researchers found that consuming Shamma significantly increased the risk of developing oral cancer by 29-fold.
Many factors contribute to this high incidence of advanced cancer stage at specialized centers. Among the causes is late consultation due to patients dismissing the signs and symptoms as inflammatory and self-resolving. Another factor is the lack of centralization of management with all centers deciding on what cancers to treat and what cancers to refer and that is a negative double edge sword; first, it leads to the majority of cases at specialized centers being advanced and with poor prognosis and secondly it means that simpler cases are treated at non-specialized centers and by non-oncology practitioners who would not treat the cases appropriately reducing their cure rates and ultimately increasing their recurrence which negatively affect the overall outcome of care in the region. Centers that do not have practitioners specializing in oral cancer care or do not have the facility to provide comprehensive treatment to their patients should take a professional stance to refer all oral cancer patients to centers that can provide that.
Several strategies can be used to detect oral cancer at an early stage, including screening high-risk populations, opportunistic screenings by general practitioners, as well as reducing the time between the diagnosis and treatment.[41] It has been shown that fast-track policies for urgent referrals for suspected cancer have been effective in reducing diagnostic intervals in several cancers since they were implemented in 2005 in the UK. Head and neck cancer patients, for example, have experienced a 21-day reduction in diagnostic intervals.[42]
In conclusion, this study reflects the high prevalence of advanced oral cancer cases in Saudi Arabia as experienced by an oral and maxillofacial surgery practice and it highlights the need for more collaboration between the centers to ensure timely diagnosis and referral of oral cancer patients.
None.
None.
None.
None.
|
||||||||