Deniz Publication
Clinical Cancer Investigation Journal
ISSN Print: 2278-1668, Online: 2278-0513
ISSN Print: 2278-1668, Online: 2278-0513
Metachronous Carcinoma at Colostomy Site Post Abdominoperineal Resection – A Rare Presentation Case Report
Muhammed Huzaifa1, Ankita Singh1, Vaibhav Aggarwal1, Anita Dhar1*
1Department of Surgical Disciplines, All India Institute of Medical Sciences, New Delhi, India.
Abstract
Adenocarcinoma at the colostomy site rarely occurs after abdominopelvic resection (APR), only a handful of cases are reported in the literature. In absence of biopsy such growth may masquerade as hyperplasia or granulation tissue at stomal edges, leading to diagnostic dilemmas. We report an unusual case of a gentleman in his late 50s who underwent abdominoperineal resection for rectal cancer following which he presented with stomal site growth without distant metastasis 12 years later. In view of the absence of distant metastasis, segmental colonic resection with 2 cm skin margin and revision colostomy was performed with a plan of adjuvant therapy thereafter. Though carcinoma at the colostomy site is uncommon, careful stomal observation and examination for surveillance should be done during each follow-up and we suggest early biopsy and colonoscopy in case of suspicion. Segmental colonic resection with skin margin and adjuvant therapy is the preferred option in such presentations.
Keywords: Abdominoperineal resection, Stomal site growth, Metachronous carcinoma, Segmental colonic resection
Isolated growth at the colostomy is rarely encountered in clinical practice.[1] Such growth may masquerade as hyperplasia or granulation tissue at stomal edges, leading to diagnostic dilemmas in the absence of a biopsy.[2] Due to its rarity, no definite etiology or management protocol is known for such occurrences. Here we report a case of a gentleman in his late 50s who underwent abdominoperineal resection (APR) for rectal cancer following which he developed stomal growth without distant metastasis 12 years later.
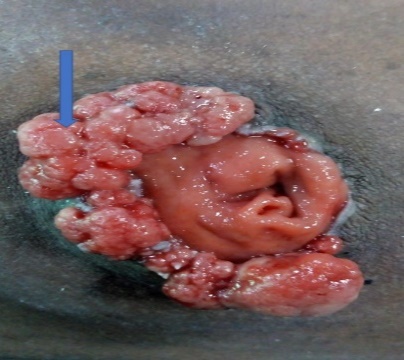
A gentleman in his late 50s, with a performance status of ECOG-1, had undergone APR with microscopically free margins (pT3N0M0) for rectal carcinoma. He had received adjuvant chemoradiation and was lost to follow-up. 12 years later, he presented with hard growth at stoma for 8 years for which no medical consultation was sought. There was no history of abdominal pain, distention, decreased stomal output, or bleeding from the stomal mass. He has no family history of malignancy. On examination, a circumferential, non-constricting hard, nodular, indurated growth was present between the eight to three ‘o’clock position (Figure 1).
|
|
|
Figure 1. Irregular, polypoidal, circumferential, nodular growth arising from the sigmoid colostomy. |
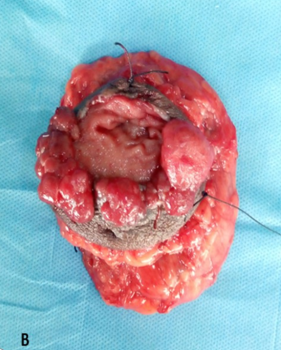
A biopsy was obtained from the lesion which revealed adenocarcinoma. Routine blood workup liver and kidney functions were within normal range. Colonoscopy showed no synchronous lesions. Contrast-enhanced computed tomography (CECT) abdomen and pelvis and positron emission tomography (PET) scan demonstrated no metastasis (Figure 2). In view of isolated growth at descending colostomy without metastasis and consultation with the oncology team, exploratory laparotomy with segmental resection of proximal 5cm of colon and mesocolon along with surrounding 2cm of circumferential skin
|
|
Figure 2. CECT abdomen showing stomal growth |
|
|
a) |
|
|
b) |
Figure 3. (a and b): Specimen of Wide local excision of stoma with 2 cm circumferential skin margin and 5cm colonic margin. |
Uncommon incidence of stomal site adenocarcinoma may lead to diagnostic delay. To our knowledge, two cases have been reported in the literature in which stomal obstruction was managed conservatively with manual and finger dilation for at least a year until the definitive diagnosis of carcinoma was established by biopsy. [3, 5] In this case, growth at the stoma site started four years after the primary resection of the tumor, but the patient presented 8 years later when a larger stoma bag was required. Delayed diagnosis is detrimental, and we must educate stoma care nurses and patients about such occurrences. Moreover, we should keep a low threshold for biopsy for suspicious clinical presentations such as obstructed stomas.
In the literature review, we found no consensus regarding the treatment of stomal site carcinoma. In general, the oncological outcomes are poor with a median survival of 30 months with a range from 6 to 84 months in such patients. [4, 6] A review of 10 such cases in literature by Davey et al. reports Segmental resection of the colon with revision colostomy as the preferred option along with adjuvant therapy.[4] Furthermore, Lymph node dissection decreases recurrence due to remnant microcarcinoma in the lymph node.
Carcinoma at the colostomy site is uncommon, careful stomal observation and examination for surveillance should be done during each follow-up and we suggest early biopsy and colonoscopy in case of suspicion. We must also educate stoma care nurses and patients about the possibility of stomal site growth which aids in early presentation. Segmental colonic resection with skin margin and adjuvant therapy is the preferred option in such presentations.
None.
None.
None.
None.
|
||||||||