|
|
|
|
Effects of Almond Porridge, Grape Extract, and Pea Syrup on Fatigue Severity of Patients with COVID-19
Ali Ghandaali1, Mozhgan Mehri Ardestani1, Saeid Hadi2, Fatemeh Nejatbakhsh3,4, Vahid Hadi2, Mohammad Hassan Kazemi-Galougahi5, Seyed Mahdi Mirghazanfari6*
1Department of Persian Medicine, Faculty of Medicine, AJA University of Medical Sciences, Tehran, Iran. 2Department of Health, School of Medicine, AJA University of Medical Sciences, Tehran, Iran. 3Department of Traditional Medicine, School of Persian Medicine, Tehran University of Medical Sciences, Tehran, Iran. 4Food Microbiology Research Center, Tehran University of Medical Sciences, Tehran, Iran. 5Department of Social Medicine, Faculty of Medicine, Aja University of Medical Sciences, Tehran, Iran. 6Department of Physiology and Iranian Medicine, School of Medicine, AJA University of Medical Sciences, Tehran, Iran.
Abstract
AJA Hospital in Tehran, Iran, will host this randomized, double-blind, placebo-controlled clinical study from March through December 2022. Almond porridge, grape extract, and pea syrup (AGP combination) + routine care and placebo + routine care groups were created at random from patients with COVID-19. During his or her stay in the hospital, the patient had a mixture of almond porridge and grape extract around 10 o'clock that contained 25 grams of almonds and 8 ccs of grape extract. Additionally, during the hospital stay, 30 grams of chickpeas were included in the snack at 16 o'clock. The Fatigue Assessment Scale (FAS) was used to evaluate patients at baseline, discharge, three months, and six months. The 6-month duration of the experiment was successfully completed by 75 patients in the AGP group and 71 individuals in the placebo group. Baseline and discharge FAS scores were used to compare patients in the two experimental groups. At the month 3 (p<0.001) and month 6 (p<0.001) visits, the AGP group, however, had a substantially lower FAS score. From baseline through months 3 and 6, the FAS score in the AGP considerably decreased (p <0.001) and declined (p <0.001) more than in the placebo group. Repeated measures analysis confirmed this and found a significant time-x-treatment interaction impact for AGP on the FAS score (F=13.029; ηp2=0.083; P<0.001). Finally, results revealed that after discharge, patients in the AGP group had significantly decreased C-reactive protein (CRP) levels (p = 0.021).
Keywords: COVID-19, Fatigue, Almond porridge, Grape extract, Pea syrup
A severe public health issue that affects a large population and results in a wide range of symptoms is the coronavirus disease 2019 (COVID-19) pandemic. One of the signs and symptoms that are most prevalent during acute COVID-19, which can continue for up to 4 weeks after the infection begins, is severe tiredness.[1-3] Symptoms of COVID-19 are referred to as post-Acute Sequelae of SARS-CoV-2 Infection (PASC), post-COVID-19 Syndrome, long COVID, or long-Haul COVID when they persist for more than 12 weeks without being explained by another condition.[4] Severe fatigue was rapidly suspected to be one of the pandemic's most frequent long-term side effects.[5-7] In actuality, both patients who required hospitalization after acute COVID-19 and those who did not require hospitalization after COVID-19 [8-11] report feeling fatigued 6–12 months afterwards. According to studies,[12-14] 20% of people with various coronavirus infections, including Extreme Acute Respiratory Syndrome (SARS), Middle East Respiratory Syndrome (MERS), and other infectious diseases, including Q-fever, have persistent post-infectious extreme exhaustion. Extreme weariness following COVID-19 may affect millions of people, leading to long-term health concerns, disability, significant disease-related expenditures, and a lower quality of life.[15] There are hundreds of millions of COVID-19 instances that have been confirmed worldwide. This necessitates an investigation into preventive or therapeutic interventions for post-COVID-19 fatigue.[16]
The most likely cause of weariness during the acute stage of an infectious disease is an adaptive reaction to the infection.[17] Most people recover once the illness has subsided. However, a small percentage of patients still experience fatigue. Severe fatigue that lasts longer than six months after infection and negatively affects a patient's functionality, quality of life, and involvement in society is known as post-infectious chronic fatigue.[18]
It is unknown what causes fatigue to persist, although several processes, such as cytokine dysregulation or neuro-inflammation, have been proposed.[19, 20] It has been proposed that COVID-19-related fatigue might be associated with imbalanced inflammatory conditions and increased oxidative stress.[21] Thus, interventions leading to decreased inflammation and oxidative stress are potential areas of interest to treat or prevent COVID-19-related fatigue. From the beginning of the COVID-19 pandemic, complementary and alternative medicine interventions have been used as alternative options to treat symptoms of COVID-19.[22] Food and vegetable ingredients, such as almonds, grapes, and peas, have vast antioxidant and anti-inflammatory properties. In this regard, Pownall et al. have demonstrated that enzymatic protein hydrolysate fractions of pea seed (Pisum sativum L.) have strong antioxidant properties.[23] Moreover, research has exhibited strong free radical-scavenging and antioxidant activities for different species of grapes, which could be used as healthy sources of natural antioxidants to prevent several disorders induced by oxidative stress, like cardiovascular disease and cancer.[24, 25] Furthermore, it has been demonstrated that polyphenols in almond skins or seed modulates plasma biomarkers of oxidative stress in healthy humans.[26] Therefore, these alternative interventions might be beneficial for treating fatigue after COVID-19.
Although prior research has concentrated on the management of chronic fatigue post-COVID-19 months after the onset of the disease, preventive interventions during the acute phase of COVID-19 may be a more preferable option, resulting in both a reduction in levels of fatigue immediately following the onset of the disease and a decreased risk of developing chronic fatigue over the long term. This trial's main goal is to determine if consuming a concoction of almond porridge, grape extract, and pea syrup (the AGP combination) reduces mean tiredness severity scores during hospitalization and at 3- and 6-month follow-ups in comparison to standard treatment. Determine if AGP combination therapy improves COVID-19 symptoms, balances laboratory values, and shortens hospital stays are the secondary objectives.
At AJA Hospital (AJA University of Medical Sciences, Tehran, Iran), from March to December 2022, a single-center, randomized, double-blind, placebo-controlled clinical study will be conducted on inpatients with COVID-19. All participants gave their written informed consent after being told of their ability to withdraw from the research at any time without having to give a reason or experience any disruption in their access to healthcare. Two parallel AGP and placebo groups were randomly assigned to eligible patients. Patients were evaluated at the beginning, after discharge, and after three and six months. The ethical guidelines of the Declaration of Helsinki and its later revisions were followed in the conduct of this experiment.[1] The AJA University of Medical Sciences' institutional review board (IRB) gave its approval to the study's protocol (IR.AJAUMS.REC.1400.322). The registration number for this trial is IRCT20220228054150N1 in the Iranian Registry of Clinical Trials.
Participants
People with a confirmed diagnosis of COVID-19, aged 18 to 65, participated in this experiment, were hospitalized for treatment, and had a score >30 on the Fatigue Assessment Scale (FAS). Included patients presented with fever (T>38) and at least one of the following symptoms and had positive results on the nasopharyngeal polymerase chain reaction (PCR) test for SARS-COV-2: respiratory rate >24, headache or myalgia, cough, 2) anosmia or hyposmia, 3) headache. The exclusion criteria of the study were: 1) intubation or intensive care unit (ICU) hospitalization, 2) respiratory distress, 3) hospital stay<2 days, 4) severe nausea or vomiting, 5) pregnancy or lactation, 6) smoking, 7) using any other herbal medicine within past 3 months, 8) diabetes with insulin requirements, hepatitis, or congestive heart failure.
Interventions
The AGP and placebo groups got the same standard of treatment. During the patient's stay in the hospital, a snack of 25 grams of almond porridge and 8 ccs of grape extract was provided to them in a single-use container at 10 o'clock. Additionally, during the hospital stay, chickpeas (containing 30 grams of chickpeas) were provided in a disposable container with the snack at 16 o'clock. The placebo was provided to the control group at 10 and 16 o'clock and resembled the intervention in terms of form, flavor, color, and fragrance. No other medication was allowed for trial participants.
Outcomes and tools
The FAS was used to measure the degree of tiredness at three different points: baseline, discharge, and follow-up sessions at three and six months. A 10-item fatigue questionnaire called the FAS is used to assess exhaustion. Five questions correspond to physical exhaustion, and five questions correspond to mental exhaustion. The raters had an inter-reliability of >90% and were skilled doctors. Additionally, blood samples from patients were obtained at baseline and discharge, and laboratory tests such as the complete blood count and inflammatory markers were performed. Moreover, the clinical symptoms of patients were recorded.
Clinical symptoms and laboratory indicators made up the trial's secondary outcome measures, while the FAS score served as its major end measure.
Adverse events
During the trial, patients and a professional rater both reported adverse events. All patients were urged to call a 24-hour, accessible phone line at any time to notify their doctors of any unanticipated adverse effects. The researcher asked open-ended questions regarding any potential adverse effects at each session.
Sample size
Based on pilot research, we calculated the sample size, taking an effect size of 0.23 for the FAS score into account. With an 80 percent power, a 5% 2-sided significance level, and a 20 percent attrition rate, the trial's total sample size was 160 patients (80 in each arm).
Randomization and blinding
AGP and placebo groups were randomly assigned to the patients at a ratio of 1:1. Each participant was assigned a unique random code. The study's principal investigator performed the randomization and allocation using permuted block randomization using blocks of size 4. At the conclusion of the research, the confidential allocations were made public. The placebo mixes were identical to the AGP. Separate researchers who were blinded to allocations carried out the randomizations, administration, evaluation, data input, and statistical analysis.
Statistical methods
The data were analyzed using the Statistical Package of Social Science Software (SPSS version 20, IBM Company, USA). Categorical variables are represented as frequency (%), whereas continuous variables are represented as mean (standard deviation). The FAS scores between the AGP and placebo groups from the study's beginning to its endpoint were compared using an independent T-test. The Mann-Whitney U test was used to compare Likert variables (such as headache) between groups. The study groups (AGP versus placebo) were assumed to be the between-subject variable (treatment), and the scores at baseline and follow-up sessions were assumed to be the within-subject factor (time) when analyzing the time treatment effects for FAS scores between the two groups using the general linear model (GLM) repeated measures method. Mauchly's test of sphericity was used to determine if the Greenhouse-Geisser correction for degrees of freedom was necessary. As the effect size, partial eta squared (ηp2) was taken into account.[27] Statistics were deemed significant at a P-value of 0.05 or below.
Demographic and clinical characteristics of participants
The inclusion/exclusion criteria were run against 225 inpatients with COVID-19 in total. 95 individuals were eliminated, and the 160 patients who remained were randomly divided into two groups and given 1:1 ratio of either AGP or placebo mixes (Figure 1). During their hospital stays, nine patients in the AGP group and five patients in the placebo group were moved to the ICU and were subsequently eliminated. No patient passed away or withdrew from the trial after being released. After a 6-month period, 75 patients in the AGP group and 71 patients in the placebo group had finished the experiment. Table 1 displays the participant's demographic and clinical features at baseline. Age, sex, and length of hospital stay were compared between AGP and placebo patients.
|
|
|
Figure 1. Flow diagram of the study |
Table 1. Baseline characteristics of the patients in two trial groups |
|||
|
|
Intervention group (n=75) |
Placebo group (n=71) |
P-value |
|
Age [years; mean (SD)] |
48.05 (13.2) |
47.58 (14.5) |
0.836a |
|
Sex [n (%)] |
|
|
0.828b |
|
53 (70.7%) |
49 (69%) |
|
|
22 (29.3%) |
22 (31%) |
|
|
Hospital stay [days; mean (SD)] |
6.59 (1.2) |
7.04 (1.6) |
0.142c |
P-value of <0.05 was considered statistically significant.
SD: standard deviation
a Independent T-test
b Chi-square test
c Mann–Whitney U test
Outcomes
Primary outcome measure
FAS score
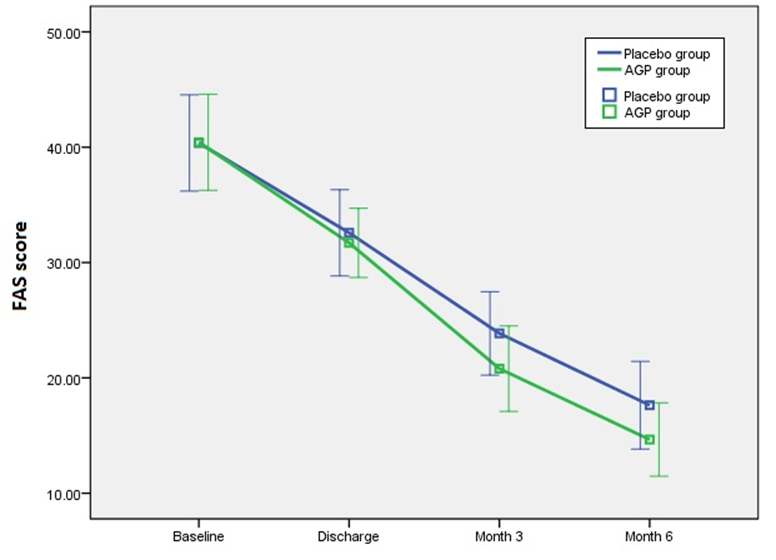
Table 2 displays the baseline, discharge, and two follow-up visits FAS ratings for the AGP and placebo groups. Based on the patients' baseline and discharge FAS total scores, the two study groups' patients were equivalent. However, during the month 3 (p<0.001) and month 6 (p<0.001) visits, the AGP group had substantially lower FAS scores. From baseline to months 3 and 6, the FAS score in the AGP considerably decreased more than in the placebo group (p<0.001) and month 3 (p<0.001), respectively (Figure 2). GLM repeated measures analysis revealed a significant time treatment interaction effect for AGP on the FAS score (F=13.029; ηp2=0.083; P<0.001) in accordance.
Table 2. Comparison of FAS scores between the two trial groups |
|||
|
FAS |
Intervention group (n=75) |
Placebo group (n=71) |
P-value |
|
Baseline |
40.43 (4.16) |
40.37 (4.18) |
0.930a |
|
After discharge |
31.71 (3.00) |
32.58 (3.74) |
0.081b |
|
3 months after discharge |
20.80 (3.70) |
23.86 (3.62) |
<0.001b |
|
6 months after discharge |
14.65 (3.19) |
17.63 (3.80) |
<0.001a |
|
Change from baseline to discharge |
8.72 (4.29) |
7.79 (3.24) |
0.265b |
|
Change from baseline to month 3 |
19.63 (4.50) |
16.51 (3.78) |
<0.001a |
|
Change from baseline to month 6 |
25.77 (4.58) |
22.73 (5.21) |
<0.001a |
P-value of < 0.05 was considered statistically significant; Data are shown as mean (standard deviation).
a Independent T-test
b Mann–Whitney U test
|
|
|
Figure 2. Comparison of FAS scores [mean (standard deviation)] between the AGP and placebo groups |
Secondary outcome measures
Signs and symptoms
Table 3 demonstrates that there was no significant difference in temperatures across groups, O2 saturation, presence of cough, productive cough, or diarrhea, and severity of headache and musculoskeletal pain at baseline or discharge.
Table 3. Comparison of vital signs and clinical symptoms in trial groups |
||||
|
|
Time points/periods |
Intervention group (n=75) |
Placebo group (n=71) |
P-value |
|
Temperature |
Baseline |
38.07 (0.47) |
38.05 (0.49) |
0.789 a |
|
Discharge |
37.31 (0.11) |
37.32 (0.14) |
0.977 c |
|
|
O2 |
Baseline |
89.59 (2.61) |
90.08 (2.95) |
0.281 a |
|
Discharge |
96.28 (1.28) |
96.62 (1.42) |
0.227 c |
|
|
Cough |
Baseline |
75 (100%) |
67 (94.4%) |
0.053d |
|
Discharge |
65 (86.7%) |
63 (88.7%) |
0.704 b |
|
|
Discharge in days |
6.20 (1.34) |
6.21 (2.07) |
0.213 c |
|
|
Productive cough |
Baseline |
51 (68.0%) |
48 (67.6%) |
0.959 b |
|
Discharge |
8 (8.0%) |
9 (12.7%) |
0.351 b |
|
|
Discharge in days |
1.89 (2.11) |
2.15 (2.32) |
0.602 c |
|
|
Diarrhea |
Baseline |
27 (36%) |
25 (35.2%) |
0.921 b |
|
Discharge |
20 (26.7%) |
17 (23.9%) |
0.705 b |
|
|
Discharge in days |
1.21 (2.01) |
1.85 (3.02) |
0.670 c |
|
|
Headache |
Baseline |
1.39 (1.48) |
1.06 (1.16) |
0.278 c |
|
Discharge |
0.29 (0.49) |
0.30 (0.49) |
0.980 c |
|
|
Discharge in days |
1.47 (1.99) |
2.14 (2.65) |
0.375 c |
|
|
Musculoskeletal pain |
Baseline |
3.33 (1.34) |
3.13 (1.45) |
0.406 c |
|
Discharge |
2.00 (0.97) |
1.85 (1.15) |
0.454 c |
|
|
Discharge in days |
6.24 (1.28) |
6.68 (1.61) |
0.167 c |
|
P-value of < 0.05 was considered statistically significant; Data are shown as mean (standard deviation) or frequency (%).
a Independent T-test
b Chi-square test
c Mann–Whitney U test
d Fisher's exact test
Laboratory parameters
A baseline and discharge measurement of laboratory values were performed. The baseline and discharge levels of every laboratory parameter, including ESR, WBC, hemoglobin, platelets, AST, ALT, creatinine, LDH, and albumin, were compared across patients in the two study groups. The AGP group, however, had considerably lower CRP levels at discharge, according to the results (p = 0.021) (Table 4).
Table 4. Comparison of laboratory parameters between the two trial groups |
||||
|
|
Time points/periods |
Intervention group (n=75) |
Placebo group (n=71) |
P-value |
|
CRP (mg/l) |
Baseline |
57.07 (38.13) |
56.32 (38.36) |
0.481b |
|
Discharge |
12.69 (3.38) |
15.04 (6.71) |
0.021a |
|
|
ESR (mm/h) |
Baseline |
52.27 (13.60) |
52.80 (13.0.) |
0.809a |
|
Discharge |
22.28 (4.47) |
22.51 (4.63) |
0.764a |
|
|
WBC (n/ul) |
Baseline |
7610.7 (1834.1) |
7747.9 (1597.8) |
0.695a |
|
Discharge |
5236.0 (804.1) |
5287.3 (770.3) |
0.582b |
|
|
Neutrophil (%) |
Baseline |
62.24 (5.04) |
61.37 (4.80) |
0.286a |
|
Discharge |
62.20 (3.70) |
61.37 (3.59) |
0.170a |
|
|
Lymphocyte (%) |
Baseline |
31.64 (7.55) |
31.10 (7.59) |
0.623b |
|
Discharge |
30.04 (4.23) |
30.17 (4.34) |
0.783b |
|
|
Hemoglobin (g/dl) |
Baseline |
15.50 (0.59) |
15.17 (0.61) |
0.776a |
|
Discharge |
15.22 (0.67) |
15.18 (0.68) |
0.697a |
|
|
Platelet (n/ul) |
Baseline |
205600 (53619) |
200282 (44295) |
0.920b |
|
Discharge |
235400 (49455) |
228451 (47007) |
0.386a |
|
|
AST (u/l) |
Baseline |
30.09 (11.95) |
30.56 (11.34) |
0.808a |
|
Discharge |
27.07 (9.70) |
27.51 (9.86) |
0.786a |
|
|
ALT (u/l) |
Baseline |
29.60 (9.61) |
29.70 (10.07) |
0.949a |
|
Discharge |
26.83 (9.60) |
26.45 (9.79) |
0.870a |
|
|
Creatinine (mg/dl) |
Baseline |
1.20 (0.54) |
1.19 (0.48) |
0.641b |
|
Discharge |
1.08 (0.25) |
1.07 (0.25) |
0.842b |
|
|
LDH (iu/l) |
Baseline |
500.80 (357.27) |
497.39 (354.11) |
0.810b |
|
Discharge |
167.73 (34.08) |
164.58 (34.69) |
0.431b |
|
|
Albumin (g/dl) |
Baseline |
4.61 (0.44) |
4.61 (0.46) |
0.993a |
|
Discharge |
4.65 (0.45) |
4.66 (0.46) |
0.909a |
|
P-value of < 0.05 was considered statistically significant; Data are shown as mean (standard deviation).
a Independent T-test
b Mann–Whitney U test
Clinical complications and side effects
There were no serious or unexpected negative events recorded. No participant was disqualified due to this.
In patients with COVID-19 who have significant levels of tiredness, this study is the first randomized controlled trial to evaluate the positive effects of almond porridge, grape extract, and pea syrup in reducing the severity of the condition and clinical symptoms. The COVID-19 symptoms, hospital stay, and laboratory indicators were chosen as the secondary end measures, while FAS scores were chosen as the major outcome measure. We showed that a long-term decrease in FAS score is significantly facilitated by adjuvant medication using an AGP cocktail. In the short term (immediately following discharge), the AGP combination resulted in a greater reduction in FAS score, although it did not achieve statistical significance. In addition, we demonstrated that treatment with AGP mixture leads to decreased inflammatory conditions as represented by decreased CRP. However, treatment with AGP did not show any significant effect on other laboratory markers or clinical symptoms of COVID-19, such as headache, myalgia, and productive or non-productive cough. It should be noted that during the course of the trial, FAS scores significantly improved in both the intervention and placebo groups, supporting the notion that tiredness naturally decreases with normal treatment.
Despite the fact that no research has examined the benefits of almond porridge, grape extract, and pea syrup in COVID-19 patients, there are several studies showing the beneficial effects of herbal and conventional medicine in patients with COVID-19.[28, 29] Regarding fatigue, After receiving herbal medication, 242 subjects in five controlled studies reported rates of fatigue remission, including Jinhua Qinggan granule,[30] Lianhua Qingke granule,[31] Keguan-1,[32] Xuanfei Baidu Decoction,[33] and Jinyinhua Oral Liquid.[34] Their meta-analysis revealed that using herbal remedies in addition to a conventional regimen greatly reduces tiredness compared to using only a normal regimen.[28] We, here, showed that Iranian herbal medicine can lead to reduced fatigue after COVID-19 in the long run.
Post-infection fatigue is frequently observed in many viral and non-viral illness situations.[35] As was already established, post-disease fatigue affects a large number of COVID-19 patients. Rudroff et al. [36] describe coronavirus disease-related fatigue as a decline in physical or mental function as a result of effects on central, psychological, or environmental factors. These factors depend on the task a person performs, his or her environmental circumstances, and the person's physical and mental capacity. The interplay of central, psychological, or environmental components with conditional dependent factors also affects fatigue.[37]
Observational studies have shown that the symptoms of coronavirus disease persist for around 21 days after the illness begins and for as long as 4 months in some people. Anosmia and shortness of breath are the symptoms that are most commonly reported for longer than three weeks, according to research. Despite the fact that the origin and pathophysiology of tiredness after COVID-19 are not fully known, it is postulated that both cerebral and peripheral pathways play a role in its emergence. The cytokinin storm, which causes anorexia and inflammations before causing muscular atrophy, weakness, and exhaustion, may be to blame for this fatigue. Additionally, when the immune system is active, infection raises baseline energy consumption.[38] In many cases of fatigue syndrome, especially in the beginning, a high release of cytokines seems to be associated with the T-lymphocyte response. The coronavirus disease-induced immune response resembles the traditional paradigm.[39] IL-6, TNF and IL-1 are only a few examples of the proinflammatory chemokines and cytokines that are increased due to SARS-CoV-2.[40] It has been proposed that the novel coronavirus functions as a physiological stressor when combined with fatigue syndrome stressors. The paraventricular nucleus (PVN) of the hypothalamus, which contains a collection of neuronal cells that make up the brain's stress center, may be a key target for the virus. The PVN is a collection of brain regions and neural circuits that react to various physiological stresses and are crucial for the neural regulation of endocrine and autonomic stress responses. The PVN performs the roles of a stressor, an absorber, and a processor. There are many different humoral and neurological ways for stress signals to get to the PVN of the hypothalamus; among these are infections, pain, mental discomfort, and changes in the cardiovascular system brought on by physical activity.[40] Additionally, there is mounting evidence that severely harmful autoantibodies may result in corona infections. These autoantibodies may also have a major impact on the signs and symptoms of chronic tiredness in people with COVID-19. Evidence suggests that oxidative stress and inflammation might aid the developmentof fatigue after COVID-19. Thus, replacing antioxidants and vitamins might be an effective way to lessen fatigue and disease's clinical symptoms.
We hypothesized that the observed clinical effect of the AGP mixture might be through modulating inflammatory or oxidative processes. There is a bulk of evidence demonstrating the antioxidant and anti-inflammatory effects of AGP mixture (almond porridge, grape extract, and pea syrup). Almonds have been reported to be rich sources of minerals and vitamins, particularly calcium, zinc, and phosphor.[41] Additionally, phenolic substances with potent antioxidant properties may be found in almonds.[42] Furthermore, Nile et al.[42] found that extracts of grape skins and pulps had statistically significant associations between their phenolic and flavonoid content and their capacity to scavenge free radicals. Additionally, the pea is rich in antioxidants such as tannin, phenolics, and other phytochemicals, which are non-nutritive components found in peas.[43, 44] Thus, the mixture of these ingredients might lead to the clinical effects that we observed in this study.
Our study has strengths and limitations. Our study has an acceptable number of participants and relatively long follow-ups. Furthermore, the acute phase following COVID-19 infection is the main focus of our investigation. While preventative therapies in the acute phase of COVID-19 would be a more preferable choice, previous research has concentrated on the treatment of chronic tiredness post-COVID-19, months after the illness started, leading to both decreased levels of fatigue immediately after disease onset and decreased chances of developing chronic fatigue in long-term. However, because we did not examine the AGP mixture's impact on persistent tiredness following COVID-19, more research is needed in this area. Finally, we did not assess the individual effects of AGP mixture components.
This is the first randomized controlled experiment evaluating the advantages of almond porridge, grape extract, and pea syrup in reducing the degree of exhaustion and clinical symptoms in COVID-19 patients with high levels of fatigue. The current study discovered that the AGP combination has no negative effects and is helpful in lowering tiredness severity over the long term but not over the short term. It is necessary to do more research with larger sample numbers to ascertain the effects of the AGP combination on persistent tiredness following COVID-19.
Thanks to Dr. Mirghazanfari.
None.
None.
None.
|
||||||||