Deniz Publication
Clinical Cancer Investigation Journal
ISSN Print: 2278-1668, Online: 2278-0513
ISSN Print: 2278-1668, Online: 2278-0513
Chondroblastoma in a Distal Phalanx of the Great Toe – A Rare Case Report
Vijay Ghule1, Anjali Deshpande1, Sushma Gurwale1, Tushar Kambale1*, Banymeen Iqbal1
1Department of Pathology Dr. D.Y Patil Medical College, Hospital and Research center, Dr. D.Y Patil Vidyapeeth, Pimpri, Pune – 411018, India.
Abstract
Chondroblastoma is a rare benign appearing lesion arising in the epiphysis of long bones in skeletally immature individuals. It is a cartilage-producing neoplasm constituting < 1% of all bone tumors. A 16 years old girl presented to orthopedic OPD of tertiary care hospital with swelling of her left great toe for 3 years. The swelling was insidious at onset and gradually progressed to the present size of 3.5x2.5x2 cm. Radiographic examination shows an osteolytic lesion and coarse trabeculation in the distal phalanx of the great toe suggestive of a benign bone tumor. Histopathological examination showed classical features of chondroblastoma. Post-operative follow-up was uneventful and radiological examination was normal. Flat bones like the pelvis, ribs, vertebrae, scapula, and craniofacial bones are other uncommon locations. The tumor recurrence rate is increased when the tumor is having limited resection due to the site of the tumor. Turcotte et al. reported the highest recurrence rate of tumors in flat temporal bones with recurrence within 6 months to 8 years. Chondroblastoma, an uncommon primary bone tumor presenting at the distal phalanx of the great toe was extremely rare.
Keywords: Chondroblastoma, Bone tumor, Distal phalanx of great toe, Osteolytic lesion
Chondroblastoma is a rare benign appearing lesion arising in the epiphysis of long bones in skeletally immature individuals. It is a cartilage-producing neoplasm constituting < 1% of all bone tumors.[1] It may extend into metaphysis in nearly half of cases. Chondroblastoma is uncommon in short bones of the hand and feet and arises in the phalanx.[2] We report a case of chondroblastoma in a distal phalanx of the left great toe diagnosed on bone curettage followed by tumor excision.
A 16 years old girl presented to orthopedic OPD of tertiary care hospital with swelling of her left great toe for 3 years. The swelling was insidious at onset, and gradually progressed to the present size of 3.5x2.5x2 cm and overlying skin and nail were unremarkable. It was associated with pain on pressure. There was no history of trauma. No fever or any other co-morbidities were present. On systemic examination, no abnormality was detected. Complete blood count, Renal function tests, plasma glucose, and other routine laboratory investigations were within normal limits.
Radiographic examination shows an osteolytic lesion and coarse trabeculation in the distal phalanx of the great toe suggestive of a benign bone tumor (Figure 1).
|
|
|
Figure 1. A radiograph (PA and Lateral view) of the foot shows an osteolytic lesion on the distal phalanx of the left great toe. |
An incisional biopsy and curettage from the tumor were received in the department of pathology. Biopsy shows a tumor composed of islands of chondroid tissue surrounded by diffuse-lying epithelioid type cells with grooved nuclei. Few osteoclastic giant cells are noted. A diagnosis of chondroblastoma was considered. Subsequent tumor excision and disarticulation of the great toe were done and the specimen was received in the department of pathology for histopathological examination.
Grossly specimen of disarticulated left great toe measures 3.5x2.5x2 cm. Externally unremarkable skin and nail were seen.
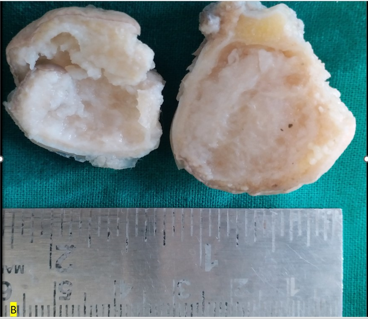
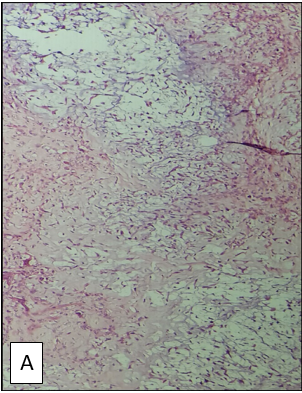
On the cut section, a well-demarcated, round, grey-white, soft, friable tumor with cystic cavities arising in the distal phalanx was seen (Figure 2). On microscopic examination, the tumor shows compact polyhedral chondroblasts with well-defined cytoplasmic borders with eosinophilic cytoplasm. Tumor cells are surrounded by lace-like patterns of hyaline matrix and chicken wire pattern of mineralization. Few osteoclastic giant cells are noted (Figure 3). This showed classical features of chondroblastoma. Post-operative follow-up was uneventful and radiological examination was normal. Informed consent from the patient was taken for publication and research purposes.
|
|
|
a) |
|
|
|
b) |
|
Figure 2. a) Disarticulated left great toe, externally unremarkable skin, and the nail as seen. b) Cut section shows a well-demarcated tumor measuring 3.5x2.5x2 cm in the distal phalanx of the great toe, greyish white with small cystic spaces. |
|
|
|
a) |
|
|
|
b) |
|
Figure 3. a) Shows sheets of polyhedral chondroblasts with pink cytoplasm, hyaline matrix, myxoid material, and chicken wire pattern of mineralization. b) Shows chondroid tissue and epithelioid cells with grooved nuclei. |
Chondroblastoma was first described by Ewing[3] as calcifying giant cell tumor. It commonly presents as a round to oval, eccentric, solitary lesion in young individuals. It commonly occurs at the proximal femur or tibia, distal femur, or proximal humerus.[4] Flat bones like the pelvis, ribs, vertebrae, scapula, and craniofacial bones are other uncommon locations.[5] It has a gritty and chalky cut surface due to calcification.[6] Chondroblastoma presenting on the distal phalanx of the great toe was unusual. Several studies have concluded that CB is derived from epiphyseal cartilage cells or in the adult population it may be due to chondroid formation by multipotential mesenchymal cells of tendon sheath as suggested by Brien et al.[7]
Other mimics like giant cell tumors, chondromyxoid fibroma, aneurysmal bone cysts, and clear cell chondrosarcoma were differentiated on a histopathological examination.[8, 9] While our case showed classical histopathological findings of chondroblastoma, other features like cortical breach, soft tissue invasion, tumor necrosis, hemosiderin deposition, and secondary aneurysmal bone cyst (ANC) formation are present in a small percentage of cases.[8, 10] Chondroblastoma is placed in the “intermediate, rarely metastasizing” category in the WHO classification of bone tumors.[11] The tumor recurrence rate is increased when the tumor is having limited resection due to the site of the tumor. Turcotte et al. reported the highest recurrence rate of tumors in flat temporal bones with a recurrence within 6 months to 8 years.
None.
None.
None.
|
||||||||