|
|
|
|
Assessment of 8-OHDG, SOD, and GPx Levels in OPMD and OSCC Patients
S. P. Ashwin1, Palati Sinduja1*, Selvaraj Jayaraman2, R Priyadharshini1
1Department of Pathology, Saveetha Dental college and hospitals, Saveetha Institute of Medical and Technical sciences (SIMATS), Saveetha university, Chennai - 600077, Tamil Nadu, India. 2Department of Biochemistry, Saveetha Dental college and Hospitals, Saveetha Institute of Medical and Technical Sciences, Saveetha University, Chennai – 600077, India.
Abstract
Free radicals define oxidative stress as the condition in which the body's antioxidant repair systems cannot keep up with the rate of cell oxidation. Oxidative stress and reactive oxygen species (free radicals) work together to damage cellular components, encourage cell neoplastic transformation, and actively affect all three stages of carcinogenesis. The most prevalent potentially cancerous conditions on the Indian subcontinent are leukoplakia and oral submucous fibrosis, which are mostly brought on by cigarette use and areca nut consumption. Assessment of 8-OHDG, SOD, and GPx levels in saliva of OPMD and OSCC patients with and without diabetes mellitus. ELISA ASSAY was used for finding the levels of 8-OHDG, SOD, and GPx. Add salivary samples and diluent 40 μL into the testing sample. Then add some 10 μL sample into the testing sample well, Cover it properly, and incubate for some 45 minutes at 37 °C. Aspirate each well and wash, repeat the process four times for a total of five washes, 1-3 minutes per time. HRP- conjugated detection antibody is added to each well. This study is one of the first attempts to find the Assessment of 8-OHDG, SOD, and GPx levels in the saliva of OPMD and OSCC patients with and without diabetes mellitus.
Keywords: Leukoplakia, Neoplastic transformation, Oral submucous fibrosis, Diabetes mellitus, Good health, Well being
When cellular oxidation outpaces the body's antioxidant repair mechanisms, the condition is known as oxidative stress, which is also referred to as free radicals. Free radicals produced as a result of oxidative stress are playing a significant role in the development of degenerative diseases like mouth cancer.[1] DNA base changes and single- and double-strand breaks are eventually caused by oxidative damage caused by highly reactive and unstable ROS. ROS and oxidative stress actively affect all three stages of carcinogenesis, interact with cellular components and cause their destruction, and encourage cell neoplastic transformation.[2]
"Not all lesions and tumors may transition to a condition like cancer rather than a modification among which some may have an elevated potential for few malignant transformations" is how oral potentially malignant disorder (OPMD) is defined.[3, 4] It suggests that while not all precancerous lesions and illnesses turn into cancer, some may have a higher chance of doing so.[5] Precancerous conditions that the WHO had previously recognized as precancers in 1978, such as oral submucous fibrosis (OSMF), actinic keratosis, and discoid lupus erythematosus, are now classified as potentially malignant disorders palatal lesions from smoking and precancerous lesions like leukoplakia.[6, 7]
The most prevalent potentially cancerous condition in India is oral submucous fibrosis, which is mostly brought on by cigarette use and areca nut consumption.[8, 9] The International Agency for Research on Cancer (IARC) expert group classified areca nuts as a known human carcinogen in 2003.[10]
One of the top 10 health risks, according to the World Health Organization, is smoking tobacco. 400 chemicals in tobacco can cause cancer, including nicotine, carbon monoxide, and aromatic hydrocarbons.[11, 12] Numerous free radicals and reactive oxygen species, including singlet oxygen (O2), hydroxyl radical (OH-), and nitric oxide, are also present in tobacco and areca nuts (NO).[13]
As premalignant conditions are linked to carcinogens like cigarettes, oral submucous fibrosis was once believed to have few connections to reactive oxygen species (ROS).[14] Free radicals related to oxygen
The study was done at the Department of General Pathology, Blue Lab, Saveetha Dental College and Hospitals, Chennai. The saliva was collected in a sterilized container from three different groups including 10 OSCC and OPMD patients with Diabetes Mellitus, 10 OSCC, OPMD patients without Diabetes Mellitus, and 10 Normal patients. Inclusion criteria were pre-operative OSCC patients and OSCC patients with diabetes mellitus. Exclusion criteria were the age and sex of the patients. The levels of TIMP1 and MMP2 in OSCC patients' salivary samples were determined using an ELISA kit. The measurements were taken with an automatic micro ELISA reader.
The measurements were transferred to an Excel sheet and all the statistical analyses were done using SPSS software version 23.0. All data were observed as mean + standard deviation.
Principle of the Assay- 8-OHDG, SOD and GPx
Sandwich enzyme-linked immune-sorbent assay technology served as the foundation for this kit. Polyclonal antibodies against 8-OHDG, SOD, and GPx were pre-coated onto 96-well plates. Additionally, as detecting antibodies, the biotin-conjugated anti-8-OHDG, SOD, and GPx polyclonal antibodies were utilized. Following the addition of the standards, test samples, and biotin-conjugated detection antibody to the wells, a wash buffer was used to clean the plates. After adding the Avidin-Biotin-Peroxidase Complex, unbound conjugates were removed using a wash buffer. We observed HRP enzymatic responses on TMB substrates. When TMB was catalyzed by HRP, a blue product was created, which later became yellow when an acidic stop solution was added. The amount of 8-OHDG sample that is caught in the plate directly relates to the density of yellow. The concentration of 8-OHDG was estimated after reading the O.D. absorbance at 450 nm in a microplate reader.
The ABC working solution and TMB substrate were equilibrated for at least 30 min at room temperature (37°C) before being added to the wells. Each test's standard curve was plotted. On the pre-coated plate, standard, test sample, and control (zero) wells were each placed, and their locations were then noted. We measured every standard and sample twice. In the standard wells, aliquot 0.1ml of the 10,000 pg/ml, 5000 pg/ml, 2500 pg/ml, 1250 pg/ml, 625 pg/ml, 313 pg/ml, and 156 pg/ml standard solutions. In the control (zero) well, 0.1 ml of the Sample/Standard diluent buffer (Kit Component 3) was introduced. The test sample wells were filled with 0.1 ml of a sufficiently diluted sample (human serum, plasma, bodily fluids, tissue lysates, or cell culture supernatants). The plate was covered and incubated for 90 minutes at 37°C. The plate was placed on absorbent filter papers or another absorbent material when the cover was removed and the contents of the plate were discarded. Anti-Human 8-OHDG antibody work solution with biotin was applied to the aforementioned wells at a concentration of 0.1 ml (standard, test sample & zero wells). Each well's bottom was filled with the solution, but the side walls were left untouched. The plate was covered and incubated for 60 minutes at 37°C. One of the following techniques was used to wash the plate three times with Wash buffer after removing the cover: Manual Washing: Do not touch the side walls of the plate as you discard the solution within. Put the plate on some absorbent material, such as filter paper. After thoroughly filling each well with Wash buffer (Kit Component 10), lightly vortex the plate on an ELISA shaker for 2 minutes, aspirate the contents and place the plate on absorbent filter sheets or another absorbent material. To get three washes, repeat this process two more times.
Automated Washing: Aspirate each well before using the Wash buffer (Kit Component 10) to wash the plate three times (overfilling wells with the buffer). Invert the plate and place it on absorbent filter paper or another absorbent material after the last wash. It is advised to set the washer for a 1-minute soak duration. Each well received 0.1 ml of the ABC working solution before the plate was covered and incubated at 37°C for 30 min. With the cover off, the plate was washed five times with a wash buffer (Kit Component 10), each time being given 1-2 minutes to sit in the wells. (For a method to wash plates, see Step 9). Each well received 90 l of TMB substrate (Kit Component 8), and the plate was covered and left to sit at 37 °C in the dark for 25–30 min. The first 3–4 wells (which contained the most concentrated Human 8–OHDG standard solutions) displayed various hues of blue, but the remaining wells lacked any discernible hue. Each well had 0.1 ml of the Stop solution added to it. and yellow color is seen. After applying the stop solution, the O.D. absorbance at 450 nm in a microplate reader was read after 30 minutes.
(The relative O.D.450) is calculated as follows: (The O.D.450 of each well) - (the O.D.450 of Zero well). The relative O.D.450 of each standard solution (Y) was plotted against the corresponding standard solution concentration to create the standard curve (X). The standard curve was interpolated to get the Human MMP-2 concentration of the samples.
In this study, we have taken the enzyme value of 8-OHDG, SOD, and GPx levels in OPMD and OSCC patients with and without diabetes mellitus. OSCC and OPMD patients with type 2 diabetes mellitus show increased oxidative stress with a decrease in antioxidant enzymes. This study proves that mean salivary 8-OHdG levels show significant differences among the other enzyme levels. Tables 1-3 shows the mean and stadand deviation of the SOD, GPx and 8- OHDG value in OPMD and OSCC patients respectively and Figures 1-3 are the graphical representation of the same.
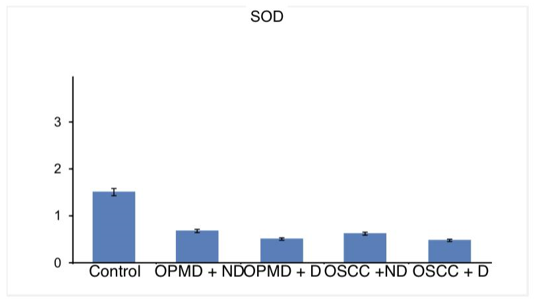
Table 1. Shows the mean and standard deviation of SOD value in OPMD and OSCC patients |
||
|
Sample |
Mean |
Standard Deviation |
|
control |
1.53 |
0 |
|
OPMD + ND |
0.695 |
0.04 |
|
OPMD + D |
0.523 |
0.02 |
|
OSCC + ND |
0.643 |
0.03 |
|
OSCC + D |
0.489 |
0.02 |
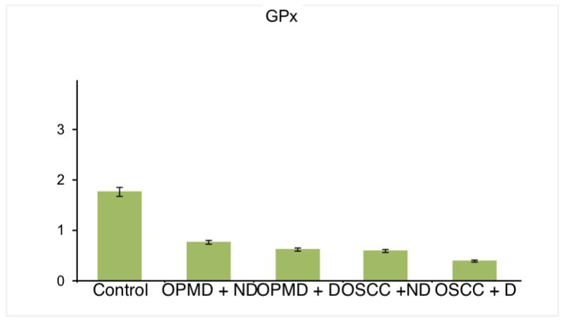
Table 2. Shows the mean and standard deviation of GPx value in OPMD and OSCC patients |
||
|
Sample |
Mean |
Standard Deviation |
|
control |
1.782 |
0 |
|
OPMD + ND |
0.767 |
0.02 |
|
OPMD + D |
0.627 |
0.02 |
|
OSCC + ND |
0.603 |
0.03 |
|
OSCC + D |
0.411 |
0.02 |
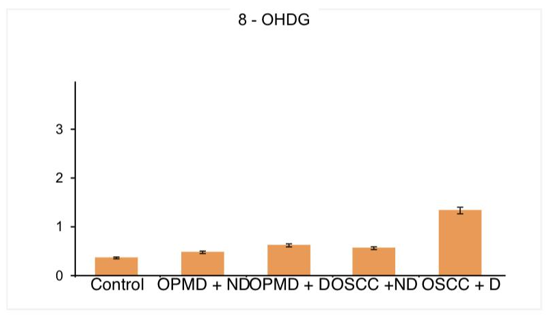
Table 3. Shows the mean and standard deviation of 8 - OHDG value in OPMD and OSCC patients. |
||
|
Sample |
Mean |
Standard deviation |
|
control |
0.376 |
0 |
|
OPMD + ND |
0.486 |
0.04 |
|
OPMD + D |
0.634 |
0.03 |
|
OSCC + ND |
0.57 |
0.02 |
|
OSCC + D |
1.35 |
0.01 |
|
|
|
Figure 1. It shows the 8-OHDG enzyme level in different patients such as control OPMD + ND, OPMD + D, OSCC + ND, OSCC + D. and it shows higher levels in OSCC patients who are diabetic. |
|
|
|
Figure 2. It shows the GPx enzyme level in different patients such as control OPMD + ND, OPMD + D, OSCC + ND, OSCC + D. and it shows the lowest level in OSCC patients who are diabetic. |
|
|
|
Figure 3. It shows the SOD enzyme level in different patients such as control OPMD + ND, OPMD + D, OSCC + ND, OSCC + D. and it shows the lowest level in OPMD patients who are diabetic. |
In this study, we have seen that OSCC and OPMD patients with type 2 diabetes mellitus show increased oxidative stress with a decrease in antioxidant enzymes. Oral potentially malignant disorders (OPMD) indicate that not every lesion and symptom under this may progress to cancer, but there is a family of structural changes, some of which may be more likely to progress to malignancy. The prevalence rate of OPMD is 0.2-0.5%, while the rate of malignant transformation is 7.6%.[5, 17]
Oral submucous fibrosis, formerly referred to as a precancerous condition, is included in the OPMD category. Arecanut has been cited as the most likely causative agent by Sinor et al. The International Agency for Research of Cancer expert group told areca nut was a known human carcinogen in 2003. The areca nut's numerous reactive oxygen and reactive nitrogen species encourage cancer-causing action in the cell. Our team has extensive knowledge and research experience that has translate into high quality publications.[18-24]
The process of oxidative stress tends to happen when the body's antioxidant defenses are unable to scavenge free radical species. DNA damage brought on by oxidative stress is possible. Such DNA damage can result in cell death, mutagenesis, and carcinogenesis. The products of the free radical species damage DNA, lipids, and proteins, and they are thought to be good indicators of oxidative stress even though measuring them is highly challenging due to their short half-lives.[25-27]
Under OPMD and OSCC conditions along with type 2 diabetes mellitus, there will be a significant increase in oxidative stress and a decrease in antioxidant enzyme levels. In this study, we found a significant decrease in antioxidant enzymes level namely Superoxide dismutase and glutathione peroxidase. Moreover, there was an increased oxidative stress marker, 8- Hydroxyguanosine. This suggests OPMD and OSCC patients with diabetes have a synergistic increase in oxidative stress contributing to the depletion of antioxidant enzymes.[28]
As OSMF and OSCC patients, the mean 8-OHdG values in saliva gradually increased from controls. This gradient increase in 8-OHdG indicates the elevated levels of DNA damage and the environment's oxidative stress under these circumstances. In their study, Totan et al. (2015) examined disease-related biomarkers in OLP patients' saliva and serum. They found 8-OHdG levels in serum and saliva from the OLP and control groups to be significantly different. In comparison to controls, 8-OHdG levels were higher in OSCC patients, and Kumar et al. (2012) hypothesized that this would make 8-OHdG a highly accurate indicator of oxidative stress in cancer.
The results of the study conclude that OSCC and OPMD patients with type 2 diabetes mellitus show increased oxidative stress with a decrease in antioxidant enzymes. It also elicits the fact that mean salivary 8-OHdG level shows significant differences between patients with OSMF and OSCC, in this OSCC showing the highest mean 8-OHdG levels. Thus salivary 8-OHdG could be used as a novel biomarker for DNA damage to assess disease progression from OSMF to OSCC.
We would like to thank Saveetha Dental College and Hospitals, Saveetha Institute of Medical and Technical Sciences, Saveetha University for providing us support to conduct the study.
None.
The present project is supported by
Saveetha Institute of Medical and Technical Sciences
Saveetha Dental College and Hospitals, Saveetha University.
The ethical approval was obtained from the Institutional Ethical Committee.
|
||||||||