Deniz Publication
Clinical Cancer Investigation Journal
ISSN Print: 2278-1668, Online: 2278-0513
ISSN Print: 2278-1668, Online: 2278-0513
3D-CRT Versus SIB IMRT Acute Toxicity Outcomes in Preoperative Concurrent Chemo-Radiotherapy for Locally Advanced Rectal Cancer
Karim Mashhour1*, Ehab Saad1, Hoda Abdelghany2, Wedad Hashem1
1Department of Clinical Oncology, Kasr Al-Ainy School of medicine, Cairo University, Egypt. 2Department of Medical Physics, Kasr Al-Ainy School of Medicine, Cairo University, Egypt.
Abstract
The primary aim of this study is to compare the acute toxicity profiles between locally advanced rectal cancer (LARC) patients treated with preoperative 3-dimensional conformal radiotherapy (3D-CRT) and simultaneous integrated intensity modulated radiation therapy (SIB-IMRT). 40 patients with LARC were equally divided into 2 groups; arm A received preoperative 3D-CRT concurrent with Capecitabine, while arm B received preoperative SIB-IMRT concurrent with Capecitabine. All patients were seen and evaluated once a week during chemo-radiation and any acute toxicity was recorded. Significantly fewer patients experienced grade 3 genitourinary toxicities in arm B vs arm A with a p-value = 0.048. Regarding grade 2 and grade 3 gastrointestinal toxicities, it was significantly higher in arm A compared to arm B with p-values of 0.043 and 0.021 respectively. There were no statically significant differences between Dmean & Dmax of the urinary bladder (UB) and small bowel (SB) in both techniques. The V45 of the UB was higher significantly in the 3D-CRT plans compared to the SIB-IMRT plans, with a p-value of 0.003. The V45 of SB was higher in the 3D-CRT arm with a p-value of 0.001. The V45 of UB & SB was statistically less in the IMRT plans compared to the 3DCRT plans. This was reflected in the toxicity profile of the patients, grade 2 GU as well as grades 2 & 3 GI toxicities were statistically of lower frequency in the IMRT group compared to the 3DCRT group.
Keywords: 3DCRT, SIB-IMRT, Genitourinary, Gastrointestinal toxicities
The current standard of care for treating locally advanced rectal cancer (LARC) patients (those with extra-peritoneal extensions).[1-3] Incorporates the usage of neoadjuvant radiotherapy (RT) alone or in addition to chemotherapy (CT).Patients with unresectable disease or those where “down-sizing” and “down-staging” are needed (cT3 mesorectal fascia (MRF) −/+ N0 of the lower rectum or cT3–4 [MRF] +/N0–2) multimodality therapy is considered a preferable option.[4]
Radiotherapy (RT) field for LARC patients should include the primary gross tumor, whole mesorectum, entire pre-sacral space, as well as regional lymph nodes. The two-D radiotherapy technique was traditionally used to cover the desired region via 3- to 4- fields. When 3DCRT (3-dimensional conformal radiotherapy) was introduced, dose coverage to the area of interest as well as sparing surrounding organs at risk (OARs) has been better.[5] Yet, avoiding the OARs using the 3D-CRT was not easy due to the horseshoe-shaped desired volume hugging the bladder and small bowel in rectal adenocarcinoma cancer patients.[6] To lower the irradiated planned volumes and doses reaching the OARs, higher RT techniques such as intensity-modulated radiotherapy (IMRT) must be used. Using the IMRT technique allows variable doses to different target volumes that can be delivered in the same fraction.
This is called simultaneous integrated boost IMRT (SIB-IMRT), which increases the dose delivered per fraction to the boost volume while keeping and maintaining the dose to the elective target volume to the minimum, providing clinical as well as dosimetric outcome superior advantages.[6, 7]
The relationship between the dose reaching the small bowel and the incidence of acute diarrhea during preoperative chemo-radiation is very obvious.[8] Many dosimetric studies have concluded that the use of IMRT inrectal cancer patients would be able to lower the dose to adjacent OARs
Moreover, several retrospective clinical studies had concluded that the use of IMRT can significantly lower the incidence of toxicity, reducing treatment breaks, as well as the need forhospitalizations.[11-14]
Before starting treatment, detailed oral and written information was provided to all patients as well as informed signed consent was a pre-requisite to enroll patients into our study. An acceptance from our local institutional research and ethical committees was obtained on the study design (N-130-2022).
Between September 2022 and February 2023, 40 patients with LARC were treated at the Kasr el Ainy Clinical Oncology department-Cairo University. The patients were equally divided into 2 groups; arm A received preoperative 3D-CRT concurrent with Capecitabine, while arm B received preoperative SIB-IMRT concurrent with Capecitabine.
The patients must have had the following inclusion criteria to be enrolled in this study: patients with pathologically confirmed rectal adenocarcinoma with clinical staging II or III. Pretreatment imaging was requested forthe patients, including a rectal dedicated magnetic resonance imaging (MRI), computed tomography (CT) scan of the chest, abdomen & pelvis, proctoscopy and/or endorectal ultrasound, clinical examination, and routine laboratory tests.
CT planning with a slice thickness of 3mm was initially performed covering the region of interest. The patients treated by 3D-CRT were aligned in the prone position while for the IMRT technique, the supine position was used. All patients in both arms were advised to drink a pre-specified amount of fluids and to hold urination one hour before the simulation process as well as before each treatment session. The target treatment volumes and doses were prescribed based on ICRU Reports 50, 62, and 83.[15, 16]
All visible primary tumors and enlarged lymph nodes were delineated as the gross target volume (GTV). An extra margin of 1 cm from the GTV represents the boost volume (CTV2) whereas the clinical target volume 1 (CTV1) encompasses the CTV2, mesorectum, and draining lymph nodes starting from L5/S1 as a superior border down to 4 cm below the tumor inferiorly. The external iliac lymph nodes were contoured in case of any gross genitor-urinary structure infiltration. In the case of levatorani muscle involvement, the ischio-rectal fossa was delineated. An additional margin of 5-10 mm was added to the CTV to account for factors such as bladder filling and bowel gas which might alter the inter-fractional variation of the target volume. Finally, a 5 mm margin was added to the CTV1 and CTV2 to account for the planning target volumes (PTV1 and PTV2), respectively.
For the patients treated by 3D-CRT, the 3 fields or 4 fields box technique wasused in treatment planning. The prescribed dose was 45Gy/25F/5weeks to PTV1 followed by a boost of 5.4Gy/3F to PTV2 with a total dose of 50.4Gy. As for the SIB-IMRT plans, 7-9 fields were used and generated using a dynamic multileaf collimator technique. The dose prescribed was 45Gy/25F/5weeks and 50Gy/25F/5weeks to PTV1 and PTV2, respectively. The treatment was delivered using 6MV photons on a linear accelerator Clinac 2100 (Varian, Palo Alto, USA).
Concerning the SIB-IMRT plans, the distribution of the dose encompassing the normal tissues outside the PTVs wasset for a rapid dose fall-off. The maximum (Dmax) dose of the bladder and small bowel outside the PTV1 and PTV2 was aimed to be kept lower than the doses prescribed. The position of the patients during the treatment course in both groups was verified once weekly using an onboard electronic portal imaging device (EPID). The dose constraints for the main organs at risk were as follows: Dmax<55Gy and V45Gy <195cc for the small bowel while for the bladder V35Gy<35% and V30Gy <50%.[17, 18]
All patients (arm A & arm B) were referred for surgical intervention within 6–8 weeks after the completion of the preoperative chemoradiotherapy.
All patients (arm A & arm B) received concomitant chemotherapy with Capecitabine during radiation therapy at a daily dose of 825 mg/m2/12 hours (excluding weekends). One of the doses was given an hour before the radiation session.
All patients were seen and evaluated once a week during chemoradiation and any acute toxicity was recorded. The acute toxicity and treatment compliance were assessed on weekly basis in accordance withthe common terminology criteria for adverse events (CTCAE) v.4.0.[19]
The comparison regarding the characteristics of the patients and the most frequently reported toxicities wasmade between the 3DCRT & IMRT groups using Fisher’s exact tests and t-tests. The final models were significant at p ≤0.05. Models were fit in R version 3.13.[20]
Between September 2022 and February 2023, 40 patients with LARC were treated at Kasr Al-Ainy Center of Clinical Oncology (NEMROCK). The patients were equally divided into 2 groups; arm A received preoperative 3D-CRT concurrent with Capecitabine, while arm B received preoperative SIB-IMRT concurrent with Capecitabine. All patient & tumor characteristics are shown in Table 1.
Table 1. illustrates thepatient and tumoral characteristics of both arms involved in the study. |
|||
|
Characteristic |
Arm A % ( n=20) 3D-CRT |
Arm B % ( n=20) IMRT |
p-value |
|
Gender |
|
|
|
|
Male |
15 (75%) |
14 (70%) |
4.45 |
|
Female |
5 (25%) |
6 (30%) |
|
|
Age, median |
60 (56-64) |
61 ( 57-65) |
0.14 |
|
ECOG Performance status |
|
|
|
|
0 |
6 (30%) |
5 (25%) |
0.62 |
|
1 |
12 (60%) |
14 (70%) |
|
|
2 |
2 (10%) |
1 (5%) |
|
|
Tumor Grade |
|
|
|
|
Well-differentiated |
2 (10%) |
2 (10%) |
0.72 |
|
Moderately differentiated |
12 (60%) |
10 (50%) |
|
|
Poorly differentiated |
4 (20%) |
4 (20%) |
|
|
Unknown |
2 (10%) |
2 (10%) |
|
|
Clinical Stage at diagnosis |
|
|
|
|
II |
10 (50%) |
9 (45%) |
0.62 |
|
III |
10 (50%) |
11 (55%) |
|
|
cT-stage |
|
|
|
|
cT2 |
5 (25%) |
4 (20%) |
0.52 |
|
cT3 |
14 (70%) |
13 (65%) |
|
|
cT4 |
1 (5%) |
3 (15%) |
|
|
cN-stage |
|
|
|
|
N0 |
2 (10%) |
3 (15%) |
0.32 |
|
N1 |
14 (70%) |
10 (50%) |
|
|
N2 |
4 (20%) |
7 (35%) |
|
|
Mesorectum |
|
|
|
|
Involved |
12 (60%) |
13 (65%) |
0.43 |
|
Not involved |
8 (40%) |
7 (35%) |
|
|
Distance from the anal verge (cm) |
|
|
|
|
< 5cm |
11 (55%) |
8 (40%) |
0.23 |
|
>5 cm |
9 (45%) |
12 (60%) |
|
|
Interrupted Radiotherapy course |
|
|
|
|
Yes |
2 (10%) |
1 (5%) |
0.53 |
|
No |
18 (90%) |
19 (95%) |
|
Regarding the median age, gender & performance status, it was balanced between both arms. Moderately differentiated carcinoma is the most grade in both arms A & B presenting 60% & 50% respectively. Fifty percent (50%) of patients in arm A werein clinical stage II, while 45% were in arm B, with an insignificant p-value. Sixty percent (60%) of patients in arm A were found to have involved mesorectum, while it was involved in 65% of patients in arm B, yet with insignificant p-value as well. The interruption of radiotherapy was more or less indifferent between the 3D-CRT & the SIB-IMRT groups (p-value 0.53).
The acute toxicity frequency rates by treatment arm aredescribed in Table 2. Although grade 1 genitourinary toxicity was numerically higher in arm B than in arm A yet it didn’t reach a significant level. Significantly fewer patients experienced grade 3 genitourinary toxicities in arm B vs arm A with a p-value = 0.048. Eighty percent of patients in arm B experienced grade 1 gastrointestinal toxicities, which was significantly higher than those with the same grade in arm A (p-value = 0.032). Regarding grade 2 and grade 3 gastrointestinal toxicities, it was significantly higher in arm A compared to arm B with p-values of 0.043 and 0.021 respectively.
No significant differences were recorded between both groups regarding the hematological, skin, and cardiac toxicities; as well as the rate of acute leakage, which occurred in 3 patients compared to 2 patients in arm A and arm B respectively.
Table 2. Shows theradiotherapy-induced adverse events encountered during the treatment course in both arms. |
|||
|
Adverse event |
Arm A % (n=20) 3D-CRT |
Arm B % (n=20) IMRT |
p-value |
|
Genito-urinary |
|
|
|
|
G0 |
1 (5%) |
1 (5%) |
1.000 |
|
G1 |
11 (55%) |
13 (65%) |
0.083 |
|
G2 |
4 (20%) |
4 (20%) |
1.000 |
|
G3 |
4 (20%) |
2 (10%) |
0.048 |
|
Gastro-intestinal |
|
|
|
|
G0 |
0 (0%) |
`0 (0%) |
1.000 |
|
G1 |
10 (50%) |
16 (80%) |
0.032 |
|
G2 |
7 (35%) |
4 (20%) |
0.043 |
|
G3 |
3 (15%) |
0 (0%) |
0.021 |
|
Hematological |
|
|
|
|
G0 |
5 (25%) |
4 (20%) |
0.073 |
|
G1 |
13 (65%) |
14 (70%) |
0.082 |
|
G2 |
2 (10%) |
2 (10%) |
1.000 |
|
G3 |
0 (0%) |
0 (0%) |
1.000 |
|
Skin |
|
|
|
|
G0 |
1 (5%) |
1 (5%) |
1.000 |
|
G1 |
15 (75%) |
12 (60%) |
0.062 |
|
G2 |
4 (20%) |
7 (35%) |
0.071 |
|
G3 |
0 (0%) |
0 (0%) |
1.000 |
|
Cardiac |
|
|
|
|
G0 |
17 (85%) |
19 (95%) |
0.093 |
|
G1 |
3 (15%) |
1 (5%) |
0.061 |
|
G2 |
0 (0%) |
0 (0%) |
1.000 |
|
G3 |
0 (0%) |
0 (0%) |
1.000 |
|
Early leakage |
|
|
|
|
Absent |
17 (85%) |
18 (90%) |
0.076 |
|
Present |
3 (15%) |
2 (10%) |
0.092 |
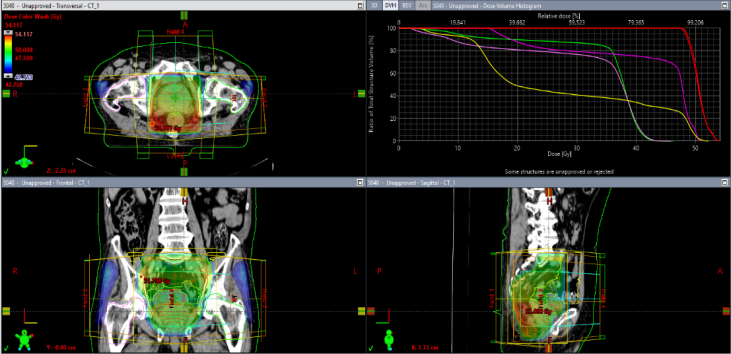
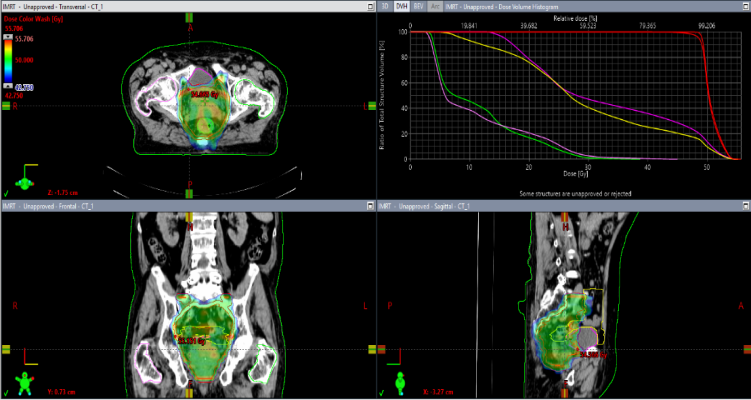
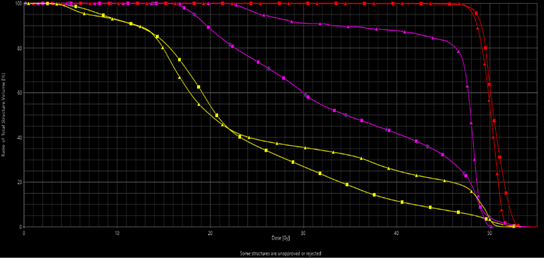
Examples of the dose distribution in 3D view are shown in Figures 1 and 2 for the 3D-CRT & SIB-IMRT techniques respectively. Figure 3 shows a DVH comparison for doses to OAR & PTV coverage for the 3D-CRT and SIB-IMRT plans.
The urinary bladder & the small bowel were OARS of interest in our study. Regarding the urinary bladder, there were no statically significant differences between Dmean&Dmax in both techniques with a p-value of 0.521 & 0.362 respectively. The V45 was significantly more in the 3D-CRT plans compared to the SIB-IMRT plans, with a p-value of 0.003. As for the small bowel, the differences in the Dmax&Dmean showed a p-value of 0.378 & 0.324. The V45 was higher in the 3D-CRT arm with a p-value of 0.001. Table 3 shows a comparison of dose-volume parameters of the bladder and small bowel between both study groups.
Table 3. Comparison of dose-volume parameters of the bladder and small bowel between the SIB-IMRT and 3D-CRT groups |
||||
|
Organ |
Parameter |
3D-CRT plan |
SIB-IMRT plan |
P-value |
|
Bladder |
Dmean (Gy) |
34.3 ± 35.5 |
33.5 ± 5.2 |
0.521 |
|
Dmax (Gy) |
48.2 ± 2.3 |
48.8 ± 5.1 |
0.362 |
|
|
V15 (cm3) |
115.4 ± 100.5 |
138.5 ± 98.1 |
0.254 |
|
|
V45 (cm3) |
31.4 ± 35.4 |
16.8 ± 17.1 |
0.003 |
|
|
Small bowel |
Dmean (Gy) |
24.5 ± 7.1 |
25.6 ± 8.4 |
0.378 |
|
Dmax (Gy) |
45.1± 9.2 |
42.9 ± 13.7 |
0.324 |
|
|
V15 (cm3) |
170 ± 158.6 |
220 ± 140.5 |
0.118 |
|
|
V45 (cm3) |
37.8 ± 44.1 |
9.5 ± 10.2 |
0.001 |
|
|
|
|
Figure 1. Dose Distribution in 3D view for the 3D-CRT plan |
|
|
|
Figure 2. Dose Distribution in 3D view for the SIB-IMRT plan |
|
|
|
Figure 3. A Comparative DVHs for PTV coverage and doses to OAR for 3D-CRT (triangles) and SIB-IMRT (squares). |
Our findings were similar and consistent with other clinical and dosimetric studies that showed lower bowel doses with IMRT and thus less gastrointestinal toxicity. Yang TJ and his team have previously found out in a small dosimetric study that women receiving CCRT for rectal cancer had experienced a higher frequency of grade 2 diarrhea commencing at week 4 of starting the treatment protocol (24% vs 11% men, p = 0.01) and patients who received 3DCRT also had higher rates of grade 2 diarrhea compared to those received IMRT (22% vs 12% respectively, p = 0.03).[14]
A retrospective clinical study done in Arizona at the Mayo Clinic concluded that patients who received the IMRT technique developed less frequent grade 2 GI diarrhea in comparison to those treated with 3D-CRT (23% IMRT versus 48% 3DCRT).[13] On the other hand, proctitis and urinary toxicity were almost equal in bothgroups. In a study conducted by Parekh et al. significantly higher rates of grade 2 GI diarrhea werenoticed with 3D-CRT (43% vs 10% IMRT, p = 0.014).[12] While grade 3 or more diarrhea was not recorded in the IMRT group, the small sample size in their study was inadequate to document those patients.
Jabbour and his colleagues underwent a study including 86 patients; IMRT had significantly decreased all grade 3 toxicities including fatigue, pain, hematological, genitourinary, and gastrointestinal symptoms. Independently, GI symptoms were not significantly less when analyzed.[11] Patients receiving combined concurrent chemotherapy experienced more grade 3 toxicities compared to those who had received single-agent chemotherapy (43% vs 11 % respectively, p = 0.009). As expected, fewerhospitalization and emergency room admission rates were observed in the IMRT patients (2% versus 14% 3DCRT, p = 0.005).
A large retrospective study conducted by Shu Y. Ng compared the acute toxicitiesamong rectal adenocarcinoma cancer patients treated with radiotherapy using IMRT versus 3D-CRT planning. The study population was very homogeneous as only preoperative primary tumors were counted; including concurrent chemotherapy using single-agent 5-fluorouracil-based and prone position in a full bladder status. They concluded that using IMRT significantly decreased grade 2 diarrhea and genitourinary toxicity during chemoradiation with a tendency to reduce proctitis as well. Although the influence of IMRT on GI and GU symptoms was not specifically limited to any subgroup, yet, patients younger than 55 years had higher chances of experiencing and having worse proctitisand thus would benefit the most from using IMRT aiming at reducing this potentially distressing acute toxicity.[21]
Regarding the doses to the OAR, our findings were matching other publications concerning the superiority of IMRT in reducing doses to the irradiated OAR. LeireArbea et al. conducted a dosimetric study comparing IMRT to 3D-CRT in cases with LARC. IMRT showed also a clear advantage over 3D-CRT in terms of bladder sparing. The volume of bladder receiving ≥ 40 Gy was almost 1/3 in cases treated with IMRT compared to the 3DCRT group (34.4 ccs vs. 94.7 cc, p < 0.05). They also found that the volume of the small bowel (SB) receiving ≥ 40 Gy with IMRT was almost 1/3 compared to that of the 3DCRT (68.9 ccs vs. 178.3 cc, p < 0.05).[9] When Duthoy and his group[22] compared 3D-CRT with intensity-modulated arc therapy (IMAT) in LARC; IMAT could significantly deliver fewer doses to the SB. A small retrospective study done by Guerrero and his team[23] comparing dosimetrically IMRT to conventional 3DCRT plans in 5 patients; showed that the SB volume receiving 45 Gy and 50 Gy was significantly decreased with IMRT. Tho and his colleagues[8] performed IMRT planning in eight LARC patients, comparing the volume of small bowel included to the 3DCRT plans. They concluded that inverse planning could reduce the median dose to the small bowel by 5.1Gy (p = 0.008).
Many dosimetric studies have concluded that the use of IMRT inrectal cancer patients would be able to lower the dose ofOARs, particularly the SB, thus decreasing the rate of diarrhea. We found out that the V45 was statistically less in the IMRT plans compared to the 3DCRT plans. This was reflected in the toxicity profile of the patients, grade 2 GU as well as grades 2 & 3 GI toxicities were statistically less frequent in the IMRT group compared to the 3DCRT group.
The Authors would like to thank Ms. Nelly M for manuscript editing.
None.
None.
An acceptance from Kasr Al-Ainy Institutional scientific and ethical committees was taken on our study design (N-130-2022). Written informed consent was a pre-requisite to enroll the patients in the study.
|
||||||||