|
|
|
|
Secondary Ovarian Malignancy in an Imatinib treated Chronic Myeloid Leukemia Patient Diagnosed on Fluid Cytology
Kaveripakam Ajay Joseph1, Sana Ahuja1, Sufian Zaheer1*
1Department of Pathology, Vardhman Mahavir Medical College and Safdarjung Hospital, New Delhi, India.
Abstract
A BCR-ABL fusion product identifies chronic myeloid leukemia as a clonal myeloproliferative tumor. Tyrosine kinase inhibitors have become more widely used to treat chronic myeloid leukemia, although there is still little known about their long-term negative effects, such as the possibility of additional cancers. The most common secondary malignancies reported in CML are localized to the gastrointestinal tract, prostate, lung, non- Hodgkins lymphoma, malignant melanoma and breast cancer. Herein, we report a case of serous papillary adenocarcinoma of the ovary in a known case of chronic myeloid leukemia on imatinib therapy for the past three years. The 46-year-old lady presented to us with massive ascites. Cytological examination revealed features of a papillary adenocarcinoma. The cytological diagnosis was further confirmed by immunohistochemistry on the cell block. Secondary ovarian adenocarcinoma following imatinib therapy for chronic myeloid leukemia is uncommon with only one case reported to date. It is important to evaluate the long-term effects of imatinib therapy especially the risk of developing secondary malignancies.
Keywords: Adenocarcinoma, Chronic myeloid leukemia, Ovarian, Secondary malignancy, Tyrosine kinase inhibitors
Chronic myeloid leukemia (CML) is a clonal myeloproliferative syndrome characterized by the t(9;22)(q34;11) chromosomal translocation. In adults, instances of this BCR-ABL (+) [Breakpoint cluster region- Abelson] myeloproliferative illness account for 15%–20% of all leukemia cases. Every year, there are 1.9 new cases of CML in 100,000 men and women.[1] Tyrosine kinase inhibitors have been added to the chronic myeloid leukemia therapy regimen, improving patient survival.[2] The efficacy and short-term adverse effects of imatinib are well known, however, data on long-term side effects is limited.[3] As a result of the declining mortality, the risk of the development of a second malignant neoplasm become significant.
The most common secondary malignancies reported in CML are localized to the gastrointestinal tract, prostate, lung, non-Hodgkins lymphoma, malignant melanoma, and breast cancer.[4-7] However, secondary ovarian cancer has been reported only by Nakazato et al. [6]
Herein, we report a case of serous papillary adenocarcinoma of the ovary in a known case of chronic myeloid leukemia on imatinib therapy for the past three years.
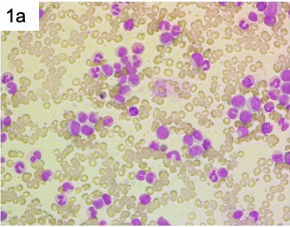
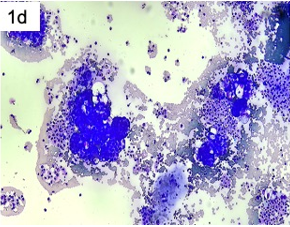
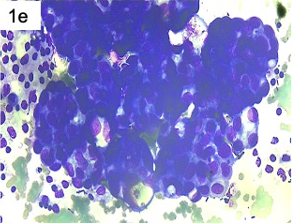
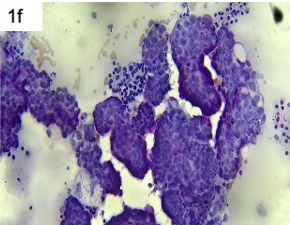
We report a 46-year-old female, a known case of BCR-ABL positive chronic myeloid leukemia on imatinib therapy for the past 3 years who presented with complaints of massive ascites. Cytocentrifuged deposits were prepared from 25 ml of the hemorrhagic and turbid ascitic fluid sample. The smears were cellular and displayed clusters of benign mesothelial cells, inflammatory cells, and three-dimensional and papillaroid pieces of malignant cells with a high nucleus-to-cytoplasmic ratio, sparse to moderate cytoplasm, and conspicuous nucleoli (Figure 1).
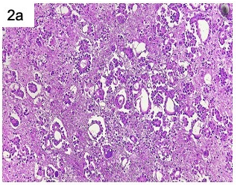
Cell block preparation was made using the alcohol-formalin method and immunohistochemistry was performed to identify the possible site of primary.[8] The cell block showed a tumor arranged as papillae with central fibrovascular cores and tumor cells exhibiting moderate pleomorphism with prominent nucleoli.
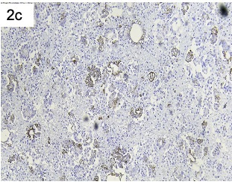
On immunohistochemistry, the cells were positive for CK7, WT1, p53 and negative for CK20 and CDX2 (Figure 2). Based on the above panel, a final diagnosis of serous papillary adenocarcinoma ovary metastasizing to ascitic fluid was made. Further, contrast enhanced computed tomography (CECT) findings were suggestive of a large right adnexal mass thus confirming the cytological diagnosis. Her CA-125 levels were also markedly elevated. Her clinical staging was International Federation of Gynecology and Obstetrics (FIGO) Stage IC for which she was taken up for debulking surgery followed by chemotherapy with docetaxel 60-75mg/m2 and carboplatin area under curve (AUC) 5-6 repeated every 3 weeks for 6 cycles. She was compliant with the treatment and tolerated the chemotherapeutic regimen well.
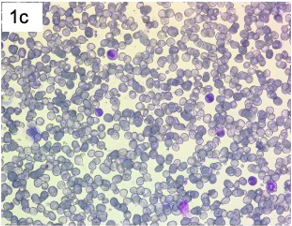
The recent peripheral blood film of the patient showed her to be in complete hematological remission.[9] Her tumor markers and ultrasound scan were also normal and she is presently asymptomatic.
|
|
|
|
a) |
b) |
|
|
|
|
c) |
d) |
|
|
|
|
e) |
f) |
|
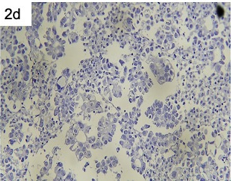
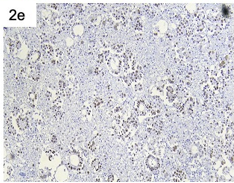
Figure 1. Peripheral film of a patient with ascitic fluid cytology smears a, b) Pre-treatment peripheral film of the patient exhibiting marked leucocytosis with a shift to left, myelocyte bulge, and basophilia [Giemsa stain; 400X, 1000X magnification] c) Present peripheral film of the patient in complete hematological remission [Giemsa stain; 400X magnification] d, e) Papillaroid fragments and 3-dimensional clusters of tumor cells exhibiting high nucleocytoplasmic ratio, coarse chromatin, and scant to moderate cytoplasm. [May Grunwald Giemsa; 200X, 400X magnification] f) Papillaroid fragments on Papanicolaou stain [200X magnification] |
|
|
|
|
a) |
b) |
|
|
|
c) |
d) |
|
|
|
e) |
f) |
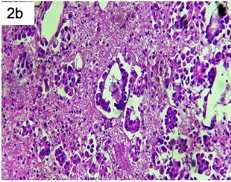
Figure 2. Cell block preparation of ascitic fluid and immunohistochemistrya, b) Cell block preparation exhibiting papillary adenocarcinoma with psammoma bodies (b) [Hematoxylin and eosin, 200X magnification] c-f) Immunohistochemistry exhibiting membranous positivity for CK7 (c), negative for CK20 (d), nuclear expression for p53 (e) and WT1 (f). [200X magnification] |
|
The treatment of CML, a clonal stem cell disorder, has profoundly improved with treatment by tyrosine kinase inhibitors.[10] The Abelson murine leukemia (ABL1) gene on chromosome 9 fuses with the breakpoint cluster region (BCR) gene on chromosome 22, which is the etiology of CML. BCR: ABL, a constitutively active tyrosine kinase, is an oncoprotein that promotes CML cell growth and survival through downstream signaling pathways including RAF (rapidly accelerated fibrosarcoma), RAS (rat sarcoma virus), STAT (signal transducer and activator of transcription), JUN kinase, and MYC (master regulator of cell cycle entry and proliferative metabolism), and is expressed as a result.[1] Imatinib provides good long-term survival, with 5-year (90%) and 8-year (88%) survival rates.[11] The most frequent causes of mortality for CML chronic phase patients having access to TKIs are progression to the advanced stage (23%), cardiovascular events (17%), and second malignancies (17%), with a 99.4-month median follow-up.[12] The mechanism of development of secondary malignancy in CML is not well defined. Imatinib's inhibitory effect on the development of dendritic cells from CD34+ progenitor cells accounts for its immunosuppressive features.[13] Due to the reduced expression of surface markers including CD1a, CD38, and MHC II on these dendritic cells, a T cell response is not stimulated. Further, tyrosine kinase inhibitors especially the newer ones, also prevent T cell proliferation by arresting T cell proliferation in G0/G1 phase.[14] Imatinib may induce neoplastic change due to interference with the DNA repair mechanisms.[15] BCR-ABL accelerates DNA damage, which encourages genomic instability and may raise a person's hereditary vulnerability to develop more malignancies.[16]
In a two-year rat carcinogenicity research, the carcinogenic impact of imatinib was first shown in a dose-dependent manner, with the no-observed effect threshold being 15 mg/kg/day. A papilloma/carcinoma of the clitoral and preputial gland was seen at a dosage of 30 mg/kg/day, which is 30% or 50% of the human dose of 400 or 800mg/day. At a dosage of 60 mg/kg/day in rats, which is 170% or 100% of the daily dose of 400 or 800 mg/kg/day in humans, urinary bladder/urethral papillomas, renal adenoma/carcinoma, adrenal medulla tumors, parathyroid adenoma, small intestine adenocarcinomas, and so on, have all been observed.[17] However, the data on the risk of secondary carcinomas post-treatment in humans is highly inconclusive.[18, 19]
The most common secondary malignancies reported in CML are localized to the gastrointestinal tract, prostate, lung, non-Hodgkins lymphoma, malignant melanoma, and breast cancer.[4-7] However, secondary ovarian cancer has been reported only by Nakazato et al.[6]
A higher risk for secondary malignancies in CML has been reported by most studies relative to the average population. Voglova and colleagues and Kumar et al. reported a 1.5 time and 30% higher risk for the development of secondary cancers respectively.[7, 20] A study conducted on the Swedish population by Gunnarson et al. found a 50% greater risk of developing secondary cancers which are in concordance with the data of several small studies.[19-24]
However, discordant findings have been observed in a few other studies. Miranda and colleagues as well as Verma and colleagues observed fewer cancers in CML patients relative to the average populace. However, Miranda et al. found significantly higher rates of non-Hodgkin’s lymphoma among CML patients.[25, 26] Also, Gugliotta et al. noted no discernible rise in secondary cancers among the CML patients on Imatinib therapy.[27]
Further, more research is required to assess the real prevalence of different secondary malignancies after imatinib therapy in chronic myeloid leukemia.[28, 29]
Secondary ovarian adenocarcinoma following imatinib therapy for chronic myeloid leukemia is uncommon with only one case reported to date. It is important to evaluate the long-term effects of imatinib therapy especially the risk of developing secondary malignancies.
None.
None.
None.
Informed patient consent was taken for publication of this report.
|
||||||||