|
|
|
|
Persistent Fetal Vasculature with Congenital Hydrocephalus: A Case Report
Abeer Saeed Hassan Osluf1*, Maged Shoukeer1, Naif Abdullah Almarzoog2
1Department of Radiology, Armed Forces Hospital, Khamis Mushait, Saudi Arabia. 2Department of Ophthalmolgy, Armed Forces Hospital, Khamis Mushait, Saudi Arabia.
Abstract
Persistent Fetal Vasculature (PFV), also known as persistent hyperplastic primary vitreous (PHPV), is a rare developmental vitreoretinal disorder. Here we present a case study of congenital hydrocephalus associated with PFV and developmental delay. P preterm baby boy of 35 weeks gestation with a birth weight of 2.135 kg, delivered by emergency cesarean section due to fetal distress. The antenatal scan showed severe ventriculomegaly (43mm). He required brief Positive Pressure Ventilation by mask and bag then admitted to NICU. CT Brain revealed hydranencephaly and fundoscopy and B-Scan Ocular Ultrasound revealed hyperechoic mass inferotemporal indicating left retinoblastoma. However, CT ORBITS later on was done and it concluded that the findings indicate left side persistent hyperplastic primary vitreous (anterior and posterior form). No mass lesions or calcifications. WES study revealed Heterozygous variant c.1802G>T p. (Gly601val) in exon 26 of the COL4A1 gene (de novo mutation). The patient stayed in NICU for 65 days, remained hemodynamically stable in room air, with sunset eyes and wide anterior fontanelle, tolerated full oral feeding well, and was discharged home. While assessing a leukocoria or microphthalmia case, PFV must be considered a differential diagnosis. Differentiating PFV from retinoblastoma can sometimes be difficult for pediatricians and ophthalmologists to diagnose. PFV often involves just one eye, coexists with microphthalmos or cataracts, and does not include calcification. advanced imaging techniques such as CT scans are very useful in such cases. thorough examinations and investigations should be conducted by the ophthalmologist.
Keywords: Persistent Fetal Vasculature (PFV), CT Brain, Management, Diagnosis
Persistent Fetal Vasculature (PFV) is an uncommon developmental vitreoretinal abnormality, formerly known as persistent hyperplastic primary vitreous (PHPV).[1, 2] It is characterized by a retrolental fibrovascular tumor brought on by problems with primary vitreous regression.[3, 4] In the first year of birth, it is the second most typical cause of acquired cataracts.[1, 5] About 90% to 95% of the time, it is unilateral and sporadic.[6, 7] It is frequently linked to other diseases including Norrie's disease, Warburg syndrome, Patau syndrome, or retinal dysplasia when bilateral.[8, 9]
Hydrocephalus is a central nervous system condition that is defined by an excessive accumulation of cerebrospinal fluid in the brain's ventricles.[10, 11] In underdeveloped nations, hydrocephalus has a considerable negative impact on health; in the US, it is thought to cost $2 billion yearly.[12, 13] Here we present a case of PFV associated with congenital hydrocephalus.[14, 15]
This is a preterm baby boy, 35 weeks gestation with a birth weight of 2.135 kg, delivered by emergency cesarean section due to fetal distress. The mother is 28 years old, G4 P2+1, the antenatal scan showed severe ventriculomegaly (43mm), a known case of hypothyroidism on oral thyroxine. Apgar Score: 6,7 & 8 at 1.5 & 10 minutes, respectively. He required brief Positive Pressure Ventilation by mask and bag then admitted to NICU.
On examination, the baby was macrocephalic, Head Circumference: 36 cm below 90th centile, wide fontanel and spaced sutures, sunken eyes and triangular face, alert, spontaneous eye opening, bilateral hazy cornea, with sluggish reactive pupils, marked head lag, hypotonic posture with weak DTR and Moro reflex.
Initially, the baby was in respiratory distress, required nasal CPAP then improved, and currently in room air, no
hepatosplenomegaly, skin rash, or skeletal abnormalities. The abdominal ultrasound was unremarkable. CBC and CRP were normal. LFTs revealed conjugated hyperbilirubinemia. Total bilirubin: 594 umol/L, Direct: 349 umol/L, AST: 136, ALT:84, GGT: 33, ALP: 170.
The ophthalmology assessment in the right eye described pupil dilated and fundal examinations showed a large preretinal vitreous hemorrhage and a pale disc. The left eye showed microphthalmia, cataract, and no fundus view.
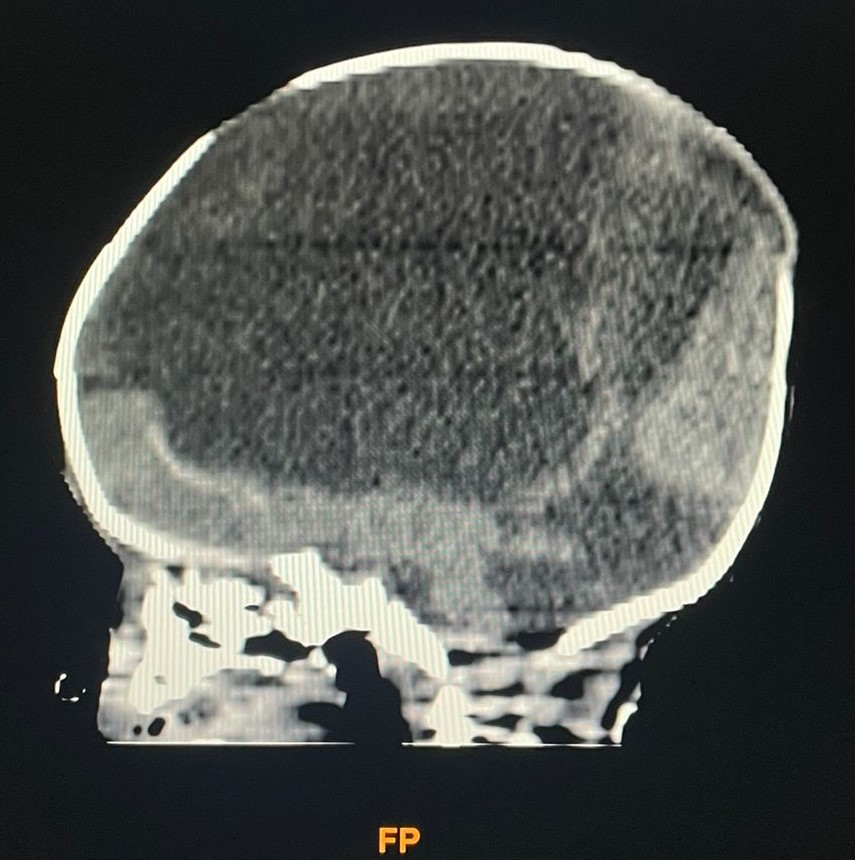
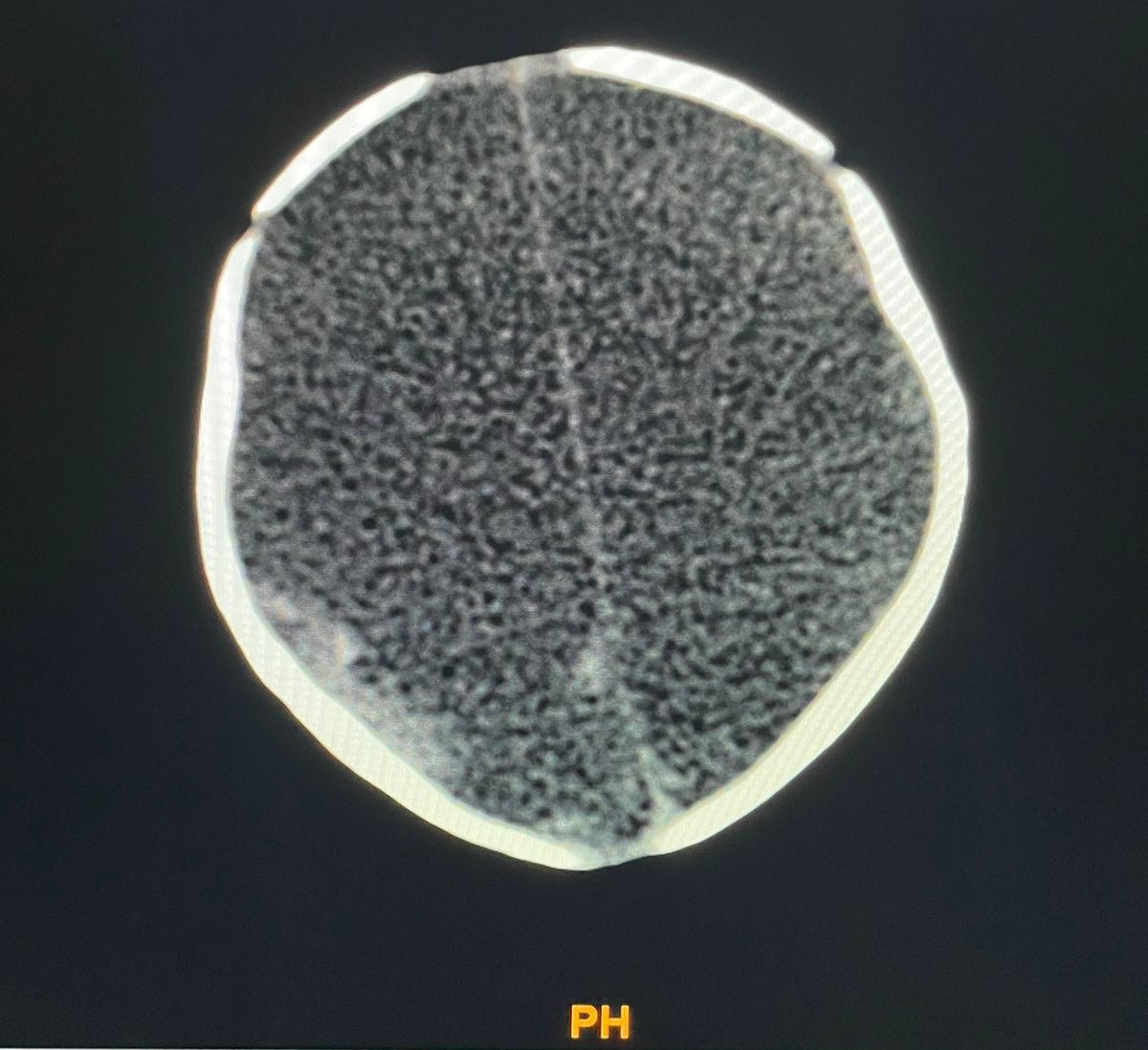
CT Brain revealed hydranencephaly (Figure 1) and fundoscopy and B-Scan Ocular Ultrasound revealed hyperechoic mass inferotemporal indicating left retinoblastoma. However, a CT scan of the orbits later was done and it concluded that the findings indicate left side persistent hyperplastic primary vitreous (anterior and posterior form). No mass lesions or calcifications (Figure 2).
The patient was transferred to a higher center and he was stable generally but on oxygen and NGT feeding, looking at an assessment of the condition of the baby and advanced genetic evaluation. WES study revealed Heterozygous variant c.1802G>T p.(Gly601val) in exon 26 of the COL4A1 gene (de novo mutation).
|
|
|
a) |
|
|
|
b) |
|
|
|
c) |
|
|
|
d) |
|
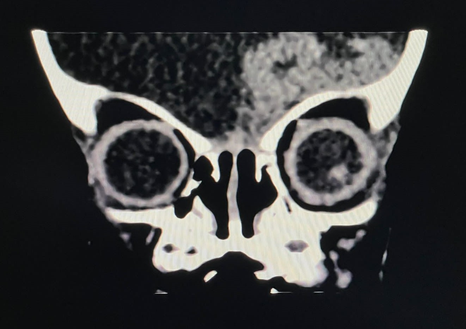
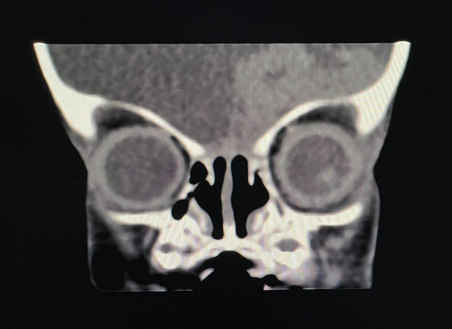
Figure 1. CT orbits showed that the left eye globe is relatively small showing a hypoplastic lens and shallow anterior chamber. Soft tissue retro-lental band is seen extending to the posterior chamber traversing the vitreous till the posterior choroidal layer. The left eye vitreous is also relatively dense. No evident calcifications or mass lesions. This right eye globe is intact. The muscle cones, optic nerves, central fat, preseptal and extra conal spaces, and lacrimal glands are of homogeneous attenuation pattern and regularly preserved boundaries bilaterally. No area of abnormal attenuation pattern or focal lesions. In addition, a normal bony orbital wall, with preserved orbital fissures, and optic foramina. The general image indicated PFV. |
|
|
|
a) |
|
|
|
b) |
|
|
|
c) |
|
|
|
d) |
|
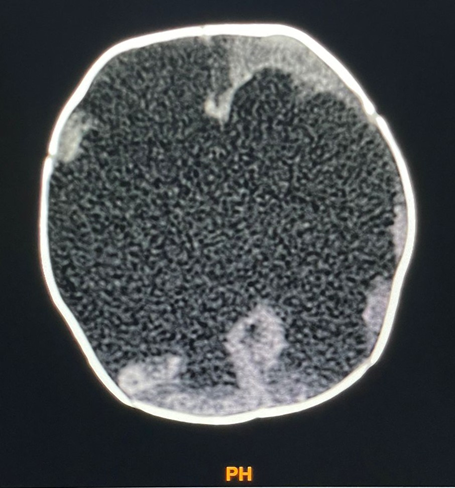
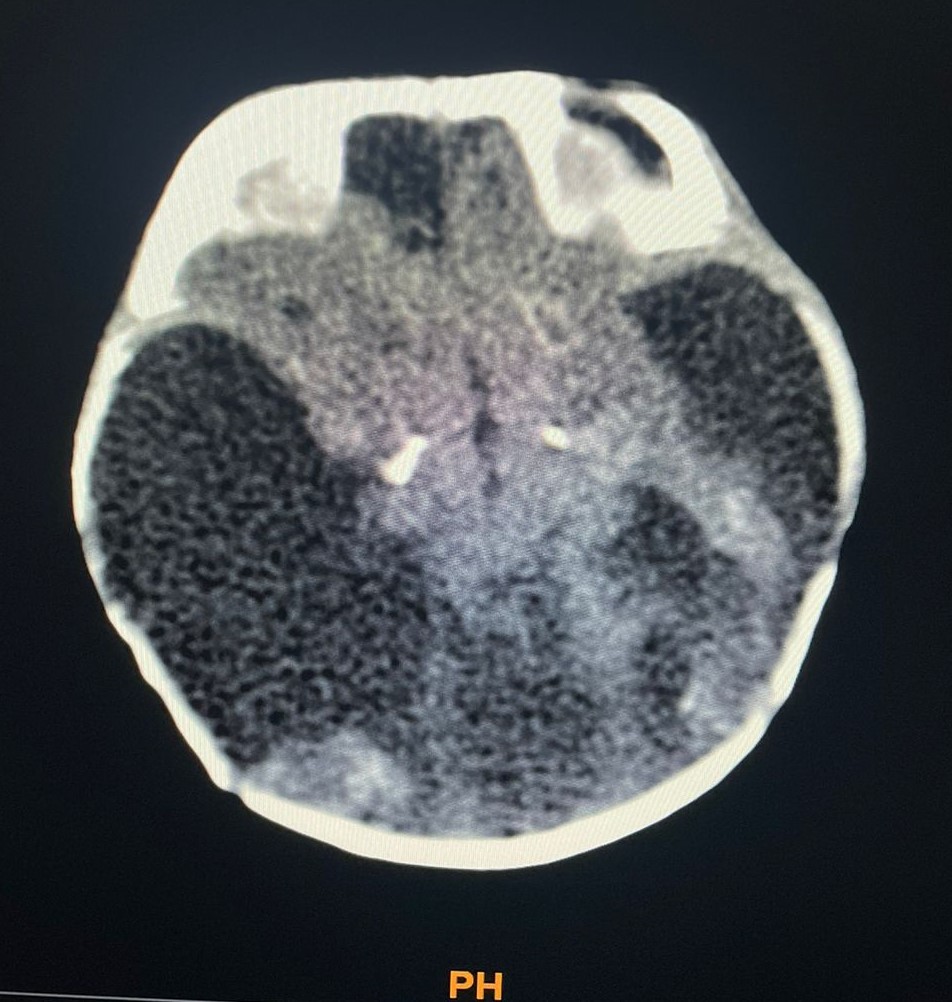
Figure 2. CT brain shows the fluid density of CSF like seen filling the skull vault with no cerebral mantle along the inner table of the skull. The falx cerebri is intact. Few remnants of the brain tissue are seen at the parietal and occipital regions showing malcalcifications. Basal ganglia calcifications are seen. The posterior fossa structure is hypoplastic, mainly the cerebellum with widened 4th ventricle. The described changes are impressive in hydrocephalus. |
The blood arteries in the embryo feed the eye as it grows. These blood vessels often disappear once the eye has fully developed. PFV has resulted when these blood vessels do not completely disappear. Clinically, leukocoria, microphthalmia, and cataract are typical symptoms. It is one of the most significant retinoblastoma differential diagnoses.[9] In our case, left retinoblastoma was our number one differential diagnosis, however, repeated ophthalmological and radiological examinations revealed that this is a case of PFV.[1] Differentiating PFV from retinoblastoma can sometimes be difficult for pediatricians and ophthalmologists to diagnose. However, while assessing a leukocoria or microphthalmia case, PFV must be taken into account as a differential diagnosis.
The ocular and orbital abnormalities in PFV, such as microphthalmia, buphthalmos, retrolental fibrosis surrounding the Cloquet canal, and retinal detachment, can be seen on a CT scan. The subretinal region is capable of detecting hyperreflective signals. Similar to our case and most of the time, there is no intraorbital or ocular calcification.[16]
To distinguish this condition from retinoblastoma on a CT scan, there must be no intraocular calcification and no microphthalmos. Because PFV often involves just one eye, coexists with microphthalmos or cataracts, and does not include calcification, it may be separated from retinoblastoma.[17]
As one of the most frequent retinoblastoma masqueraders, PFV presents in 20% of instances with suspected retinoblastoma, making it an essential differential diagnostic.[17] Leukocoria, cataracts, lengthened ciliary processes, a shallow anterior chamber, a retrolental fibrovascular membrane, and microphthalmia are the hallmark symptoms of PFV.[18] Fetal vasculature regresses throughout normal development, but in 3% of full-term children and 95% of preterm infants, it might persist and lead to various diseases.[19] An ophthalmoscopic examination is often used to diagnose PFV, however, it might be difficult to differentiate PFV from retinoblastoma. The simultaneous presence of retinoblastoma and PFV is highly uncommon. There were only 2 recorded cases of a combination of PFV and retinoblastoma, according to our knowledge.[20, 21] Therefore, thorough examinations and investigations should be conducted by the ophthalmologist.
The PFV in our case is presented in the anterior and posterior form. Based on the ocular structures affected, PFV may be categorized into three categories.[22, 23] About 25% of cases of anterior PFV are accompanied by lens opacity or posterior capsule cortical opacity, ongoing fibrovascular membrane hyperplasia behind the lens, and ciliary body elongation. The connections between the vitreous vascular membrane and the optic disc, eyeball shrinkage, and immature growth of the optic disc, macula, and retina are all factors that contribute to posterior PFV, which affects around 12% of cases. The third form is when both anterior and posterior manifestations can be seen in mixed PFV (around 63% of cases), like in our patient.
The WES study of our patient revealed a de novo mutation, a heterozygous variant c.1802G>T p.(Gly601val) in exon 26 of the COL4A1 gene. Generally, It is known that mutations in the gene COL4A1, which codes for the type IV collagen alpha 1 chain, can result in autosomal-dominant porencephaly and infantile hemiparesis.[24, 25] Porencephaly is an extremely rare disorder of the central nervous system related to the cerebrospinal fluid in the brain. Mutations in the COL4A1 gene have been found to cause COL4A1-related small cerebral vessel disease. Moreover, adult individuals with Small cerebral Vessels Disease have recently had COL4A1 mutations found in them.[25, 26] Both ischemic stroke and intracerebral hemorrhage, as well as radiological signs of lacunar infarction, leukoaraiosis, and microbleeds, are reported as clinical characteristics of this gene mutation.[26] Our patient’s CT brain showed the fluid density of CSF as seen filling the skull vault with no cerebral mantle along the inner table of the skull.
Hydrocephalus is a central nervous system condition that is defined by an excessive accumulation of cerebrospinal fluid in the brain's ventricles. Although hydrocephalus is frequently seen in children, it may happen to anybody at any age and causes serious cognitive and physical impairment. The central nervous system can be impacted by a broad range of conditions, including brain tumors, strokes, infections, and hemorrhages, which can lead to hydrocephalus. Children's hydrocephalus can result from a variety of ocular and visual diseases and has a wide range of etiologies.[27]
Untreated hydrocephalus causes ventricular dilatation and elevated intraventricular and intracranial pressure. Congenital hydrocephalus in our case coexisted with congenital anomalies of the eye. Nevertheless, hydrocephalus itself can affect the visual function and it can lead to various complications. Optic atrophy in hydrocephalus can be brought on by transsynaptic neuronal degeneration, optic nerve ischemia, optic nerve or chiasmal traction, and chiasmal compression. Visual impairment may be the only symptom of shunt malfunction and may be improved by shunt insertion. Due to their proximity to the lateral ventricles, the posterior visual pathways are susceptible to damage from ventricular dilatation. Children with hydrocephalus often have a variety of ophthalmic abnormalities, such as impaired visual acuity, visual field defects, strabismus, and ocular movement issues.[13, 27]
While assessing a leukocoria or microphthalmia case, PFV must be considered a differential diagnosis. Differentiating PFV from retinoblastoma can sometimes be difficult for pediatricians and ophthalmologists to diagnose. PFV often involves just one eye, coexists with microphthalmos or cataracts, and does not include calcification. advanced imaging techniques such as CT scans are very useful in such cases. thorough examinations and investigations should be conducted by the ophthalmologist.
Children with hydrocephalus often have a variety of ophthalmic abnormalities. Moreover, untreated hydrocephalus can lead to various visual complications.
The authors would like to acknowledge the support from the Research supervisor.
None.
None.
None.
|
||||||||