Deniz Publication
Clinical Cancer Investigation Journal
ISSN Print: 2278-1668, Online: 2278-0513
ISSN Print: 2278-1668, Online: 2278-0513
Maxillofacial Surgeons Perception of Frequency Need for Fellowship Programs for Advanced Oral Cancer in Saudi Arabia
Basem T. Jamal1,2*
1Consultant and Associate Professor Oral & Maxillofacial Surgery/Head and Neck Surgical Oncology, King AbdulAziz University, Jeddah, Saudi Arabia
2Affiliate Consultant, Oral & Maxillofacial Surgery Department, King Abdullah Medical City, Makkah, Saudi Arabia.
Abstract
Oral cancer ranks 16th worldwide. Saudi Arabia's OC rate is rising. This shows the need for oral cancer specialists. Oral and maxillofacial surgery residents cannot participate in head and neck surgical oncology and reconstructive surgery fellowship programs. No study has examined the attitude of maxillofacial surgeons, who usually are the first to encounter oral cancer, on the need for fellowship training programs in this field and that is the purpose of this study. An anonymous web-based survey was conducted, consisting of 7 questions to evaluate the current perception among practitioners on the frequency of advanced oral cancer cases, the need for a specialized training program, and the interest of these practitioners in enrolling in such a program. The survey was distributed to OMFS practitioners in different regions of Saudi Arabia. 78 practitioners completed the survey, most of whom were consultants, 49.4%. When the practitioners commented on the statement of frequently encountering oral cancer at an advanced stage due to delay in diagnosis or treatment, 43.6% strongly agreed, and 41% agreed. An overwhelming majority of practitioners believed that there is a need for oral cancer fellowship programs in Saudi Arabia, 97.4% and 61.5% of them expressed interest in applying for such a fellowship. Several Saudi Arabian institutions lack professionals skilled in advanced oral cancer surgery, and no fellowship programs in oral and maxillofacial surgery exist. OMFS practitioners are eager for fellowship training, particularly in surgical oncology.
Keywords: Oral cancer, Fellowship, Saudi Arabia, maxillofacial surgery
Oral cancer has a high prevalence worldwide and it is the 16th most common cancer in the world.[1] Globally, over 450,000 patients are diagnosed with OC each year, and the five-year survival rate is below 50%.[2, 3] Oral cancer is relatively uncommon in Arab Gulf countries, however, Saudi Arabia is an exception to this rule and there has been an increase in the incidence of OC in Saudi Arabia in recent years.[4] While a Center Tumor Registry in Saudi Arabia indicates that OC is the 5th most common cancer in males and 11th most common cancer in females,[5] the southern regions of the country in which oral cancer is much more prevalent show oral cancer is ranked first among females and second among males.[6]
Oral cancer is considered a major public health problem owing to its increasing incidence and mortality rates.[7] This adds to the burden of health care in the country being more common than in surrounding countries. The survival rate for oral squamous cell carcinoma has only marginally improved despite advancements in oncology care.[8] Some reports indicate significant improvement in the 5-year survival of oral cancer in the last 2 decades to 60% which was mainly a result of the management of cancer at its early stages.[9] However, that was noted in major centers and was not reflected in the national database and patients with poor access to health care showed significantly less improvement in survival ranging from 30-45%.[10, 11]
This highlights the demand for practitioners with expertise in the treatment of oral cancer which at most centers remains primarily surgical, although various combinations of radiotherapy and chemotherapy are included for patients with advanced disease. The American Association of Oral and Maxillofacial Surgeons (AAOMS) to help guide the management of oral cancer patients established an Oral Cancer Task Force with one of its objectives being to further the development of fellowship training programs in head and neck oncologic surgery.[12] Overall, the number of oral and
maxillofacial surgery OMFS fellowship programs in the US has increased from 7 in 2013 to 28 in 2021, and the number of candidates applying for fellowships has increased from 8 in 2013 to 31 in 2021.[13-16]
Currently, there are no fellowship training programs available to oral and maxillofacial surgery residents in the field of head and neck surgical oncology and reconstructive surgery or any other subspeciality for that matter in the Gulf region. Multiple published studies assessed the prevalence and treatment of oral cancer in Saudi Arabia as well as the perception among healthcare workers of its symptoms and features However, no study has examined the attitude of maxillofacial surgeons, who usually are the first to encounter oral cancer, on the need for fellowship training programs in this field and that is the purpose of this study.
An anonymous web-based survey was conducted on oral and maxillofacial surgery (OMFS) practitioners. The survey consisted of 7 questions to evaluate the current perception among practitioners on the frequency of advanced oral cancer cases, the need for the specialized training program, and the interest of these practitioners to enroll in such a program. The survey was distributed to OMFS practitioners in different regions of Saudi Arabia. The responses were collected over 1 month. The completed responses to the survey were tabulated and analyzed using standard statistical methodology. The questions and statements contained in the survey were designed as a 5-point Likert scale regarding practitioners’ attitudes toward oral cancer frequency and care in the country.
Practitioners were asked about their level of specialization, years of experience, frequency of encountering advanced cases of oral cancer, their opinion on the need for OMFS fellowship programs especially in oral and maxillofacial surgical oncology, and finally, their interest to pursue fellowship training in oral and maxillofacial surgical oncology.
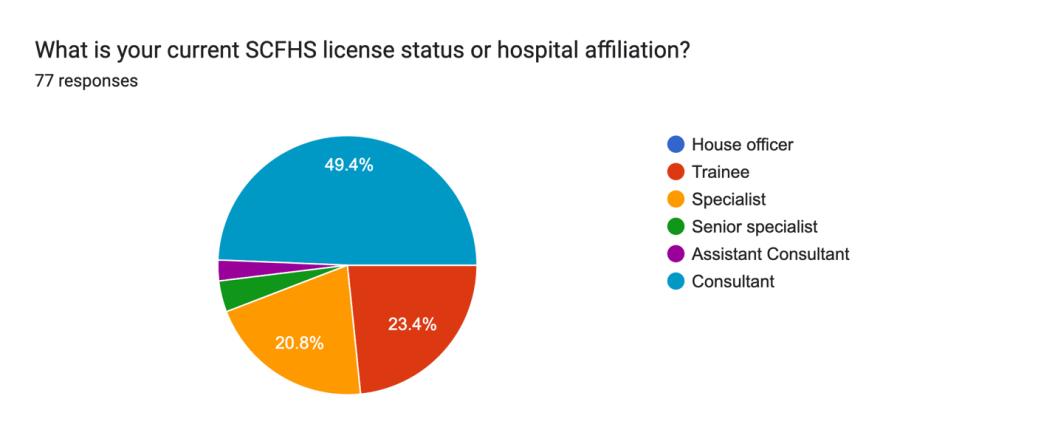
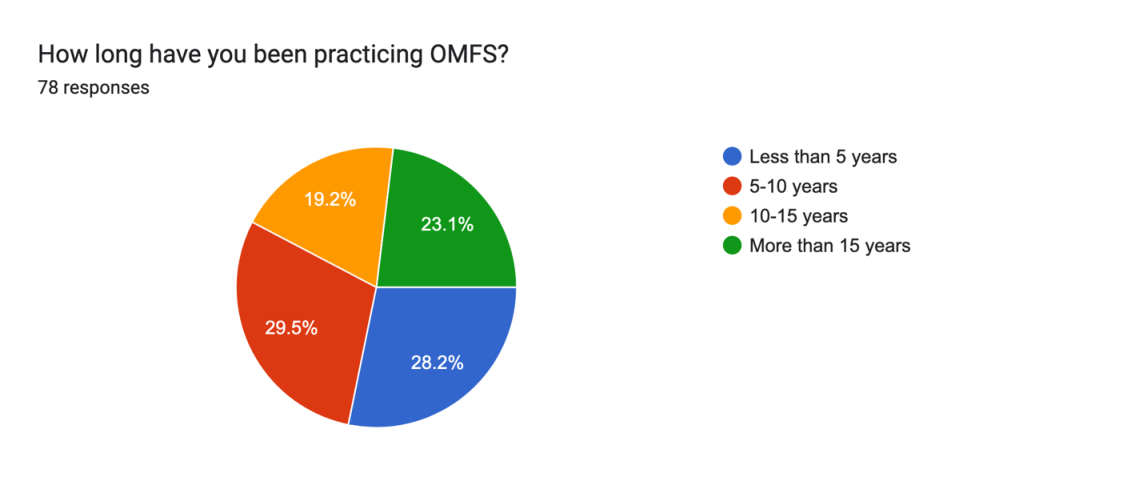
In total, 78 practitioners completed the survey. Figure 1 depicts the level of specialization of survey responders. 49.4% were consultants, 23.4% were trainees (residents), and 20.8% were specialists. There was an equal distribution of the years of experience among the participants among those who practiced less than 5 years, those who practiced between 5-10 years, those who practiced between 10-15 years, and those who practiced more than 15 years as shown in Figure 2.
|
|
|
Figure 1. Survey responders’ level of specialization in OMFS |
|
|
|
Figure 2. Survey responders’ years of practice in OMFS |
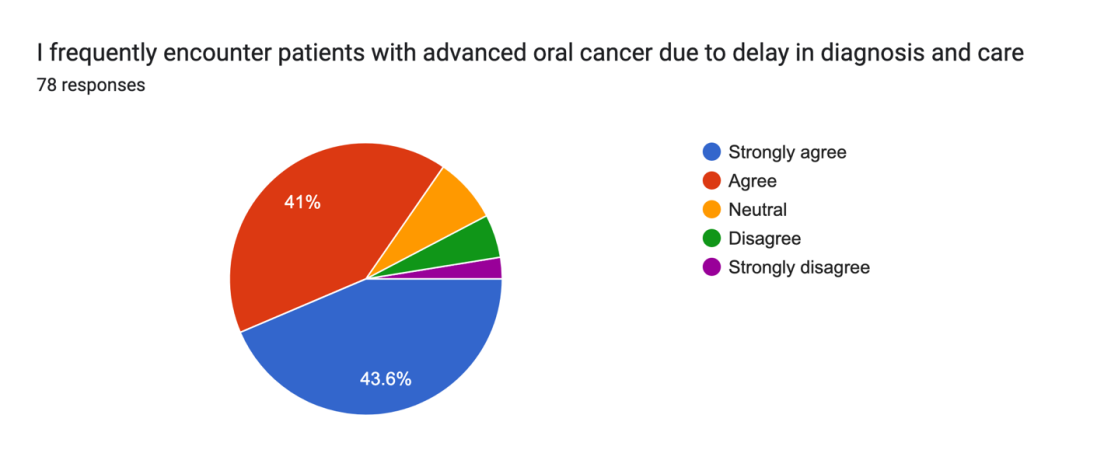
When the practitioners commented on the statement of frequently encountering oral cancer at an advanced stage due to delay in diagnosis or treatment, 43.6% strongly agreed, 41% agreed, 7.7% were neutral and 7.7% disagreed (Figure 3).
|
|
|
Figure 3. Practitioners’ response to the statement: “I frequently encounter patients with advanced oral cancer due to delay in diagnosis and care” |
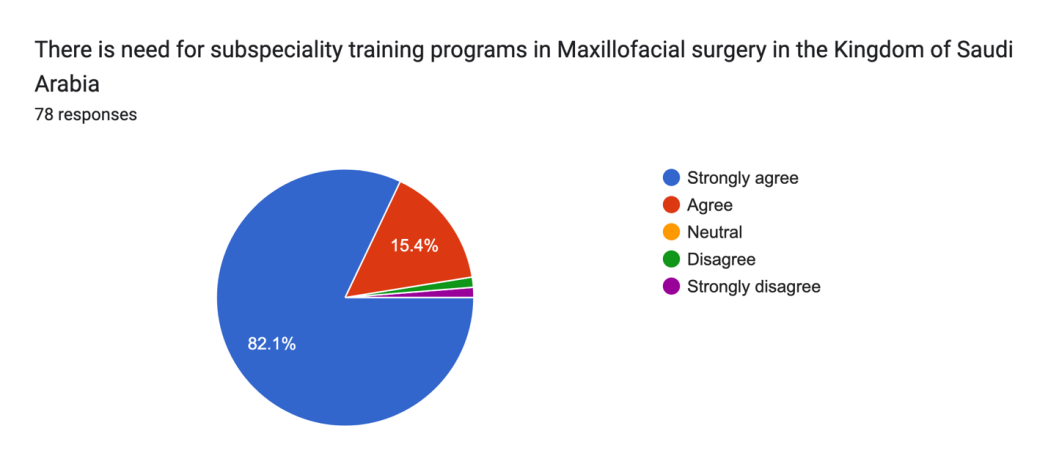
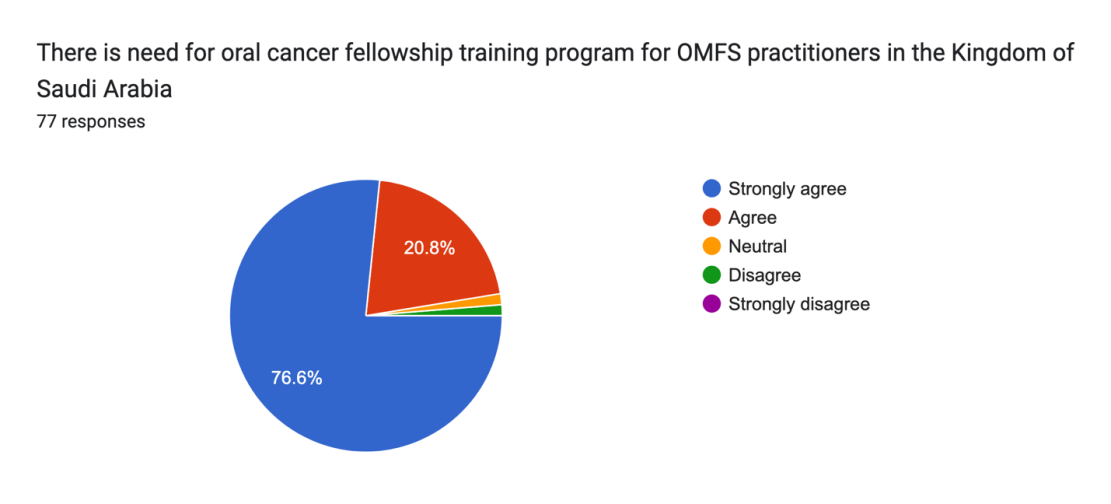
An overwhelming majority of practitioners believed that there is a need for maxillofacial surgery fellowship programs in Saudi Arabia and specifically in oral cancer care, 97.5% and 97.4% respectively as depicted in Figures 4 and 5. As expected, all participants believed that an Oral & Maxillofacial oncology fellowship program will improve the quality of oral cancer patient care in the Kingdom of Saudi Arabia.
|
|
|
Figure 4. Practitioners’ response to the need for subspeciality training programs in OMFS in Saudi Arabia |
|
|
|
Figure 5. Practitioners’ response to the need for oral cancer fellowship training program for OMFS practitioners in Saudi Arabia |
|
|
|
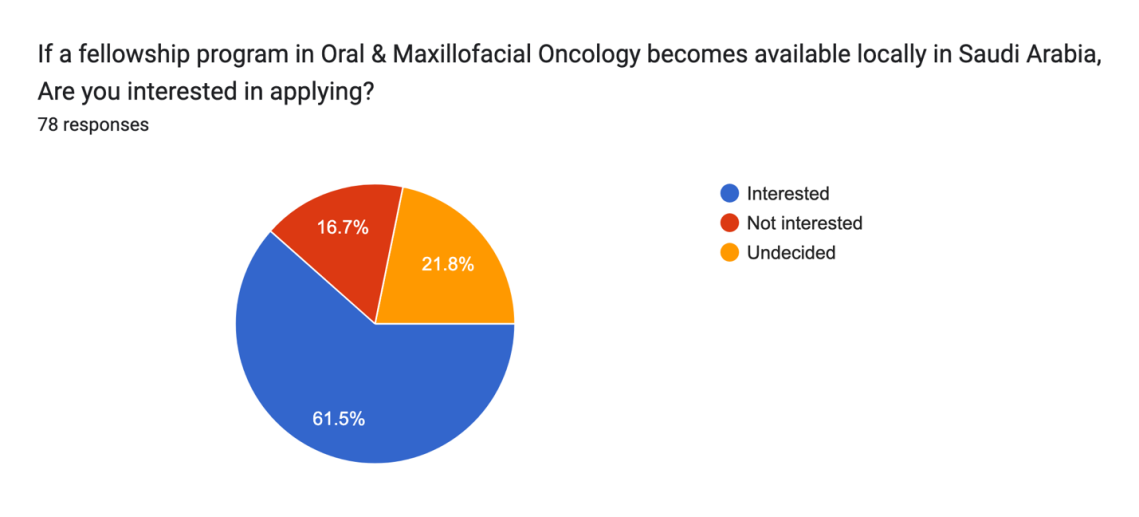
Figure 6. Practitioners’ interest in applying to an oral cancer fellowship program is available in Saudi Arabia |
Finally, to our surprise, most participants expressed interest in perusing training in oral and maxillofacial surgical oncology 61.5%. 16.7% were not interested and 21.8% were undecided Figure 6.
Fellowship programs designed to provide a comprehensive education in oral cancer surgery were developed to facilitate training in the field. An expanding number of subspecialty fellowship programs and fields are available to graduating oral and maxillofacial surgery residents including head and neck surgical oncology.[17-19] Surgical fellowships are additional periods of structured surgical training beyond residency that focus on a narrow component of advanced or unique procedures relevant to the specialty niche and usually last for 1 or 2 years. Pursuing fellowship training has been increasing in surgical disciplines, with approximately 45% of surgical residents completing fellowship programs in 2011. And this already very high percentage increased to 61.5% of the graduating residents in 2019.[20-22]
Among the factors cited by applicants for fellowships is the demand for the procedures.[23] However, the deciding factors are variable in the literature. A study of over 2000 otolaryngology residents over 8 years showed that the desire for more expertise and intellectual appeal were the most significant factors for residents to pursue fellowship training.[24] Most OMFS fellows pursue fellowship training for the same reasons as the other surgical specialties, with the desire to acquire additional skills and knowledge being their driving motivation.[17] When practitioners in the current study were asked about their interest in applying for such subspecialty training if it was available, 61.5% % showed interest despite most of the participants being consultants already.
As stated previously oral cancer is more prevalent in Saudi than in surrounding countries and the survival rates of oral cancer worldwide have been low over the past decades despite advancements in health care and technology.[8] Diagnosing oral cancer at an advanced stage is a known factor for poor prognosis and among the causes of delayed diagnosis and treatment is the lack of centers with specialized partitioners in oral cancer care. This is demonstrated in the survey by having most OMFS practitioners experiencing frequent cases of advanced oral cancer, 84%. Having trained practitioners in the surgical care of oral cancer in all major cities will ensure these patients get diagnosed and treated during the early stages of the disease. Furthermore, OMFS practitioners are perfectly suited for this role as oral cancer surgery and reconstructive surgery are intimately linked and since the foundation of OMFS, it had a rich history in reconstructive surgery.
In the US, the development of fellowship programs in various subspecialty areas of interest within oral and maxillofacial surgery was started in the 1980s by the American Association of Oral and Maxillofacial Surgeons (AAOMS) Committee for Resident Education and Training. As a result, the number of practitioners practicing head and neck surgical oncology within the field of OMFS has grown significantly.[25] A fellowship program allows the trainee to gain specialized experience in a particular patient population. As a result of the increased time and energy spent caring for these subsets of patients under supervision, patient outcomes should be improved. In addition to gaining expertise in their field of focus, the fellowship-trained surgeon will also have acquired collateral experience that can be applied to all aspects of their practice. This knowledge ranges from surgical anatomy to familiarity with surgical techniques and technological advancements.[26] Several studies have demonstrated that fellowship training has a positive impact on the quality of care provided to patients at the host institution.[27-30]
Conclusion
In conclusion, there is a lack of availability of trained clinicians in the advanced surgical care of oral cancer in many hospitals in Saudi Arabia and there are currently no fellowship programs in oral and maxillofacial surgery with an overwhelming interest among OMFS practitioners for opportunities in fellowship training, especially in oral and maxillofacial surgical oncology.
None.
None.
None.
None.
|
||||||||