|
|
|
|
Giant Cells Lesions of Oral and Maxillofacial Region – A Proposed Diagnostic Algorithm
Harpreet Kaur1, Deepika Mishra1*, Ajoy Roychoudhury2, Mehar Chand Sharma3, Ashu Seith Bhalla4, Asit Ranjan Mridha3, Aanchal Kakkar3, Rahul Yadav2, Sunny Kala1, Shashwat Mishra5
1Department of Oral Pathology and Microbiology, Centre for Dental Education and Research, All India Institute of Medical Sciences, Delhi, India. 2Department of Oral and Maxillofacial Surgery, Centre for Dental Education and Research, All India Institute of Medical Sciences, Delhi, India. 3Department of Pathology, All India Institute of Medical Sciences, Delhi, India. 4Department of Radiodiagnosis, All India Institute of Medical Sciences, Delhi, India. 5Department of Neurosurgery, All India Institute of Medical Sciences, Delhi, India.
Abstract
Multinucleated giant cells are commonly encountered in histopathology and are mostly a clue to diagnosis but sometimes pose a diagnostic confusion. The present study elucidates a case series of giant cell lesions (GCL) with emphasis on differential diagnosis and other investigations that contribute towards arriving at a final diagnosis. We also intended to devise an algorithmic approach for the accurate pathological characterization of these lesions. All the cases reported in the department from January 2018 to June 2019 were reviewed by pathologists and the total number of lesions where giant cells were diagnostic or an additional finding were included in this study. Twenty-five cases out of 1000 biopsies were diagnosed based on giant cell morphology. The most frequent lesions were central giant cell granuloma, followed by cherubism, hyperparathyroidism, peripheral giant cell granuloma, tuberculosis, and hybrid lesion. A systematic approach towards differential diagnosis for such cases and a diagnostic algorithm was devised which is being followed as per the reported spectrum of GCL. Radiological, serology, and sometimes ancillary staining techniques are essential for the accurate histopathological diagnosis of giant cell lesions. Our diagnostic algorithm helps narrow down the spectrum of investigations necessary to characterize these lesions, enabling for a swifter and more confident identification of the pathologies.
Keywords: Multinucleated giant cells, Histopathology, Central giant cell lesions, Jaws, Oral and maxillofacial gegion
Multinucleated giant cells (MGCs) are larger than normal body cells having a definite morphology and function. They consist of multiple nuclei arranged in specific morphology dispersed in the cytoplasm. MGCs of one type or another are commonly observed in the histopathology of various oral and maxillofacial pathologies.[1] MGCs were first reported in tuberculous granulomas by Rokitansky and Langhans, over a century ago.[2] Giant cell lesions (GCLs) are a group of varied lesions that contain a multitude of multinucleated, osteoclast-like giant cells within connective tissue stroma. Conventionally, these are classified as peripheral if they lie within the soft tissue or central if they lie within the jaw bone.[3]
Mohajerani et al. reported that 6.36% of the oral biopsies received in their lab were multinucleated giant cells containing lesions.[4] They are easily observed under a microscope and their presence is pathognomonic in certain lesions such as peripheral giant cell granuloma (PGCG) and giant cell fibroma.[5, 6] However, in some lesions they present a diagnostic dilemma because of uncharacteristic histopathological appearance, thus emphasizing a need for exploring clinical, radiological, and other details to arrive at a final diagnosis.[7-13] Perplexingly, sometimes, the presence of giant cells can just be an additional non-diagnostic finding.[14, 15]
This study aimed to study the prevalence of GCL pertaining to the oral and maxillofacial regions in our department and dissertate GCLs along with the differential diagnosis, special stains, and other investigations, necessary for their characterization and propose a tentative diagnostic scheme for GCLs.
To the best of our knowledge, this is the first case series aimed at ascertaining the role of giant cells as pathognomonic in diagnosis, diagnostic dilemma, or additional findings in oral lesions.
In accordance with the Helsinki declaration and relevant guidelines, we queried our records at the Department of Oral Pathology and Microbiology, from January 2018 to June 2019. We included all those cases in this study which revealed giant cells in histopathology and for which appropriate clinical, radiological, and other details were available. These were reviewed retrospectively by the six pathologists and were classified according to a working classification followed at our department. This classification was based on whether giant cells were diagnostic, coexisting with some other lesion (hybrid lesion), creating a diagnostic dilemma, or were just a supplementary finding with no role in diagnosis (Table 1). We excluded cases with insufficient information about the history, clinical photographs, radiological imaging, and other relevant investigations.
Table 1. Working classification for giant cell lesions presenting in oral and maxillofacial region based on diagnostic significance of giant cells |
|
Lesions where giant cells were pathognomonic
Benign: Giant cell tumor, Giant cell fibroma Malignant: Malignant giant cell tumor, Hodgkins lymphoma (RS cells)
|
|
Lesions where giant cell lesions presented as diagnostic dilemma / Hybrid lesions GCG can occur with a coexisting
|
|
Lesions where giant cells are present as an additional finding (non-diagnostic)
|
Results and Discussion
Table 2. Summary of 23 cases of giant cell lesions |
||||||
|
S. no. |
Age (years) / Sex |
Site |
Clinical appearance |
Radiological Features |
Other investigations |
Final diagnosis |
|
1 |
42/M |
Buccal mucosa |
Ulcer |
MRI- enhancing lesion in right masseteric space |
ZN staining, Mantoux test, culture, Interferon gamma assay –all negative, ESR raised |
Tuberculosis |
|
2 |
22/M |
Hard palate |
Swelling |
Osteolytic lesion from 16 to 21 |
Mantoux test, Interferon gamma assay, chest x ray – all negative, ESR raised |
Chronic granulomatous inflammation |
|
3 |
70/M |
Mandibular alveolus |
Soft tissue growth |
- |
PAS+ve, GMS+ve |
Histoplasmosis |
|
4 |
23/M |
Retromolar |
Soft tissue growth |
- |
- |
Peripheral giant cell granuloma |
|
5. |
28/F |
Buccal vestibule |
Soft tissue growth |
- |
- |
Peripheral giant cell granuloma |
|
6 |
46/M |
Lower lip |
Swelling |
- |
Normal ACE level, ZN staining, Mantoux test-negative, no systemic manifestations |
Orofacial granulomatosis |
|
7 |
40/M |
Mandible |
Swelling |
Multilocular radiolucency crossing midline |
Serum PTH, Ca levels- normal |
Central giant cell granuloma |
|
8 |
10/M |
Bilateral mandible |
Cherubic appearance |
Mix radiolucent –radiopaque lesion |
- |
Cherubism |
|
9 |
37/F |
Bilateral mandible, clivus |
Swelling |
Osteolytic lesions |
Serum PTH increased, Ca levels |
Hyperparathyroidism |
|
10 |
55/M |
Mandible |
Swelling |
Osteolytic lesion |
- |
Central giant cell granuloma |
|
11 |
14/M |
Mandible |
Swelling |
- |
- |
Central giant cell granuloma |
|
12 |
34/F |
Maxilla |
Swelling |
Osteolytic lesion anterior maxilla |
- |
Central giant cell granuloma |
|
13 |
18/F |
Mandible |
Swelling |
Osteolytic lesion 34-37 |
- |
Central giant cell granuloma |
|
14 |
52/M |
Mandible |
Swelling |
Osteolytic lesion ballooning out from lower border |
- |
Central giant cell granuloma |
|
15 |
42/M |
Mandible |
Swelling |
Osteolytic lesion crossing midline |
- |
Central giant cell granuloma |
|
16 |
17/F |
Mandible |
Swelling |
Osteolytic lesion wrt 24-26 |
- |
Central giant cell granuloma |
|
17 |
37/F |
Posterior mandible |
Swelling |
osteolytic lesion |
Serum PTH normal |
Central giant cell granuloma |
|
18 |
23/M |
Anterior maxilla |
Swelling |
Osteolytic lesion |
Serum PTH normal |
Central giant cell granuloma |
|
19 |
21/M |
Posterior mandible |
Swelling |
osteolytic lesion |
Serum PTH normal |
Central giant cell granuloma |
|
20 |
30/F |
Mandible |
Swelling |
Expansile osteolytic |
Serum PTH 407.2 pg/ml |
HPT related brown’s tumor |
|
21 |
06/M |
Bilateral mandible |
Cherubic appearance |
Mix radiolucent radiopaque lesion |
- |
Cherubism |
|
22 |
13/M |
Bilateral mandible |
Cherubic appearance |
Mix radiolucent radiopaque lesion |
- |
Cherubism |
|
23 |
05/M |
Maxilla and mandible |
Cherubic appearance |
Mix radiolucent radiopaque lesion |
- |
Cherubism |
|
24 |
51/M |
Mandible |
Swelling |
Multilocular radiolucency |
IHC panel- CD68+ve, panCK, Ki67, p53-ve |
OKC with giant cell granuloma |
|
25 |
6/M |
Mandible |
Swelling |
Unilocular radiolucency |
IHC panel- SATB2 +ve, MDM2, CDK4-ve, Ki67 (15%) |
Juvenile trabecular ossifying fibroma with giant cell granuloma |
Our search revealed 25 lesions among 1000 consecutive cases, where giant cells were pathognomonic while an additional 8 cases showed giant cells as a supplementary finding. Intra-osseous giant cell lesions in the order of frequency were central giant cell granuloma (11 cases), cherubism (4 cases), hyperparathyroidism (2 cases), and tubercular osteomyelitis (1 case). Peripheral giant cell lesions included peripheral giant cell granuloma (2 cases), microbial giant cell lesions (2 cases: 1 case of tuberculosis and histoplasmosis each), orofacial granulomatosis (1 case), and 2 hybrid lesions. Out of these 25 patients, eighteen were males and seven were females aged 10-70 years (Table 2). One case of each diagnosis, presenting with characteristic clinical, radiology, and/or histopathology is discussed below.
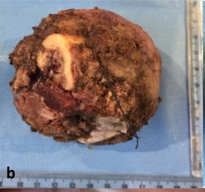
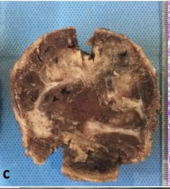
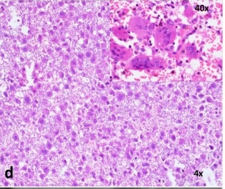
Case 1: A 52-year-old male patient was presented with swelling in the mandibular anterior region of the jaw for 1 year and 6 months. On examination, there was bony hard swelling extending from the 35th to 46th region. Orthopantomogram (OPG) revealed extensive radiolucent lesion ballooning out from the lower border of the anterior mandible. A provisional diagnosis of central giant cell granuloma and ameloblastoma was considered. Microscopy revealed compactly arranged fibrovascular stroma consisting of the abundant spindle to stellate-shaped fibroblasts with interspersed numerous multinucleated giant cells (4-20 nuclei), dense bundles of collagen fibers, and numerous endothelial-lined budding capillaries (Figure 1).
Investigations: Serum PTH, calcium, phosphorus, and alkaline phosphatase were within normal limits.
Differential diagnosis: Histopathological differential diagnosis of central giant cell granuloma, brown tumor of hyperparathyroidism (HPT), aneurysmal bone cyst, cherubism, and giant cell tumor (GCT) were considered.
GCT is a benign but locally aggressive tumor of stromal cells that occurs mostly in long bones and rarely in jaws. Histopathologically, it shows a uniform and diffuse distribution of macrophages and osteoclast-like giant cells with relatively more nuclei in the background of stromal mononuclear cells. These cells can occasionally show increased mitosis, however, usually there is no marked atypia.[5] The lack of such features eliminated the possibility of GCT. Normal PTH and calcium levels in the present case excluded hyperparathyroidism. Cherubism occurs at a young age with symmetrical bilateral involvement of jaws thus it was excluded. An aneurysmal bone cyst is characterized by large sinusoidal spaces lined by connective tissue with a focal distribution of MGCs. Surgical notes are very important for the diagnosis of this entity which revealed a blood-soaked sponge appearance.[6] Further, as the present case did not show necrosis, increased mitosis, abnormal mitosis, and cytological atypia, the malignant giant cell tumor was excluded. After ruling out all of these lesions, a final diagnosis of central giant cell granuloma (CGCG) was given.
|
|
|
|
|
|
|
a) |
b) |
c) |
d) |
e) |
|
|
|
|
|
|
|
f) |
g) |
h) |
i) |
j) |
|
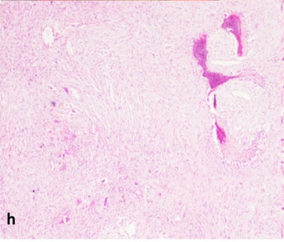
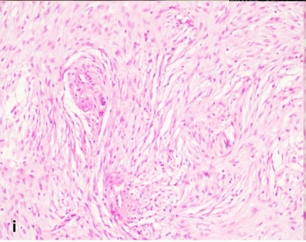
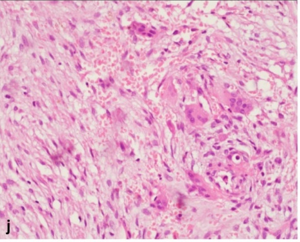
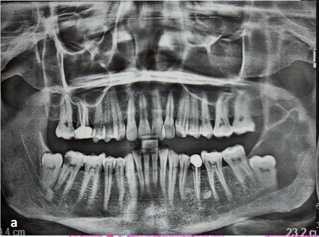
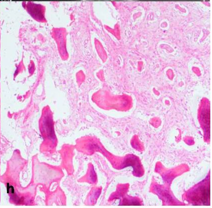
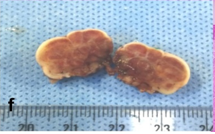
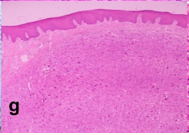
Figure 1. Case 1-Central giant cell granuloma(a-d) presenting as radiolucent lesion of anterior mandible(a). Gross showed hemorrhagic areas(b,c). Histopathology showed MGCs (H&E;4X;inset40X)(d). Case 2-Cherubism(e-j). Presented with bilateral swelling(e,f), mixed radiolucent-radiopaque lesion(h), histopathologicaly with osteoid(h;H&E;4X), perivascular eosinophilic cuffing (i;10X) and MGCs (j;40X). |
||||
Case 2: A 10-year-old female was presented with swelling in right and left cheek region giving a cherubic appearance that had grown slowly in the last year. On examination, there was diffuse bony hard swelling in the mandibular alveolus and bilateral rami. Orthopantomogram revealed a mixed radiolucent-radiopaque lesion in the bilateral rami of the mandible with mixed dentition. CBCT scan showed similar features as in OPG with a developing lesion in the right maxillary molar region. Bilateral incisional biopsies revealed loose to dense fibro cellular stroma showing perivascular eosinophilic cuffing, multinucleated osteoclastic giant cells with minimal inflammatory infiltrate, few myxomatous areas, and reactive osteoid formation lined by osteoblasts (Figure 1). All other giant cell lesions were excluded based on young age and bilateral mandibular presentation. So, the final diagnosis of cherubism was confirmed.
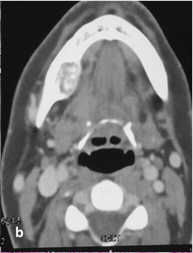
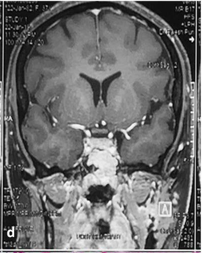
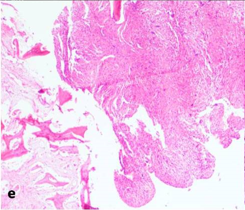
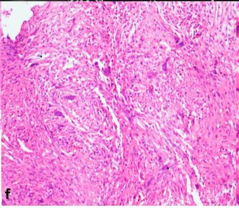
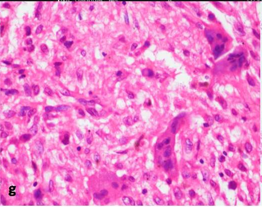
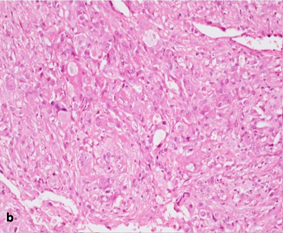
Case 3: A 37-year-old lady was presented with multiple multilocular lesions on the bilateral mandible and clivus region. CECT and PNS view showed an expansile multiloculated cystic lesion with inner body destruction noted in the body of the right and left mandible with bone remodeling and thinning of the inner cortex adjacent to 1st and 2nd molar teeth. MRI revealed another lesion in the anterior part of the clivus bulging into sphenoid sinuses with thinning of diaphragmatic sellae. Microscopy from left and right mandibular lesions and a clival tumor revealed compactly arranged fibrovascular stroma intermixed with numerous multinucleated giant cells. Intervening stroma shows abundant hemorrhagic areas and focal sinusoidal spaces. Few areas show active osteoid formation in the form of trabeculae in varying stages of maturation with osteoblastic rimming (Figure 2).
|
|
|
|
|
|
a) |
b) |
c) |
d) |
|
|
|
|
|
|
e) |
f) |
g) |
h) |
|
Figure 2. Case 3- Hyperparathyroidism (a-h). OPG shows an osteolytic lesion in the left ramus (a) and CECT shows osteolytic lesions in the left and right mandible (b,c). MRI revealed a diffuse lesion in the clivus (d). Histopathology showed giant cells with abundant bone formation(e-h; H&E;4X,10X,40X,4X). |
|||
Investigations: Serum parathormone (PTH) levels were found to be high (81.1pg/ml) but serum calcium was normal.
Differential diagnosis: Histopathological differential diagnosis of hyperparathyroidism, aneurysmal bone cyst, and hybrid lesion of ossifying fibroma with giant cell granuloma were considered. Due to multiple lesions in the mandible and skull, polyostotic fibrous dysplasia was also considered. The radiology of the case did not show well circumscribed mixed radiopaque-radiolucent lesion thus ruling out ossifying fibroma with giant cell granuloma. Similarly, the absence of peau-d'orange appearance in radiology and the absence of the Chinese letter appearance of woven bone in histopathology ruled out polyostotic fibrous dysplasia.
On the basis of multiple osteolytic lesions and high PTH levels, the final diagnosis of hyperparathyroidism-related brown tumor was established.
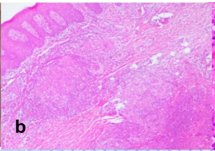
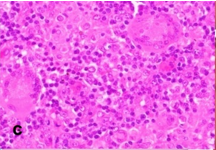
Case 4: A 42-year-old male was presented with a painless ulcer on the right retromolar trigone of 3 months. On examination, there was an enlargement of the right submandibular lymph nodes, which were matted and firm in consistency. A provisional diagnosis of traumatic ulcer and differential diagnosis of tubercular ulcer and malignant ulcer was considered. MRI revealed an enhancing lesion in the right masseteric space involving the right medial pterygoid muscle. Microscopy revealed hypercellular stroma showing multiple focal areas of collection of inflammatory cells intermixed with multinucleated giant cells resembling Langhans giant cells surrounded by a zone of fibrosis. High power showed the presence of 7-15 nuclei in the giant cell, histiocytes, lymphocytes, and plasma cells within the granuloma-like areas, and abundant blood vessels with perivascular inflammatory infiltrate primarily composed of plasma cells (Figure 3).
|
|
|
|
|
|
a) |
b) |
c) |
d) |
|
|
|
|
|
|
e) |
f) |
g) |
h) |
|
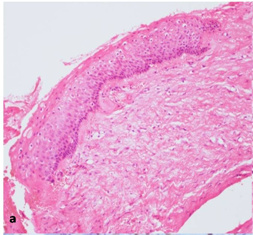
Figure 3. Case 4-Tuberculosis ulcer (a-d). Clinical presentation (a). Photomicrograph showing Langhans-type giant cells (b,c; H&E;4X,40X). Healed lesion (d). Case 5 -Peripheral giant cell granuloma(e-h). Lobular gross specimen and hemorrhagic cut surface (e,f). Photomicrograph showing epithelium with multinucleated giant cells (g,h; H&E;4X,40X). |
|||
Other investigations: Ziehl Neelsen staining was negative for any mycobacterium. PAS stain was unremarkable.
Differential diagnosis: Presence of granulomatous inflammation histopathologically excluded traumatic and malignant ulcers. Histopathological differentials were tuberculosis, sarcoidosis, foreign body granuloma, and fungal granulomatous inflammation. The absence of a foreign body in histopathological sections and no foreign body giant cells ruled out foreign body granulomas. The lack of multisystem involvement, absence of eosinophilia, and normal Angiotensin Converting Enzyme (ACE) levels were unsupportive of sarcoidosis. Fungal granulomatous inflammations were excluded by negative PAS staining and the non-visualization of fungal organisms. The final diagnosis of tuberculosis was suggested in view of histological findings, epidemiological preponderance, and positive culture reports.
The patient was referred to a pneumologist for further examination and management. Mantoux test, culture tests, and interferon-gamma assay were positive for M. tuberculosis. The patient was started on a standard anti-tubercular regimen. The patient was kept on regular follow up and complete healing of the lesion was observed on follow-up (Figure 3).
Case 5: A 23-year-old male was presented with growth in the left retromolar region for 6 months. A gross examination showed a well-circumscribed lesion with a nodular cut surface. Histopathology revealed parakeratinized stratified squamous epithelium encircling a loose fibro-angiomatous stroma with aggregates of MGCs separated by a band of normal fibro collagenous connective tissue. High power showed multiple aggregates of MGCs containing 5-12 nuclei within eosinophilic cytoplasm, active fibroblasts, dilated and engorged blood vessels and intense chronic inflammatory cell infiltrate. The diagnosis of peripheral giant cell granuloma was given (Figure 3).
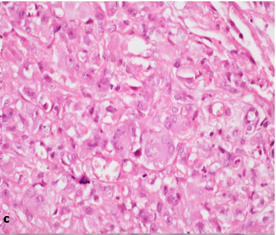
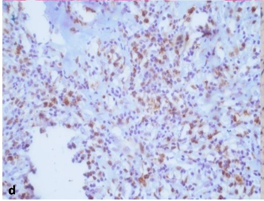
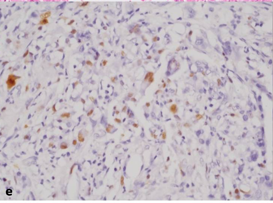
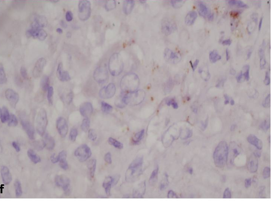
Case 6: 51-year-old male with diffuse swelling on the right side of the mandible. There is a history of two cyst enucleation and extraction of 48th tooth in 2005 and 47th in 2012. On examination, there was diffuse swelling on the mandible angle, body, and ramus region causing obliteration of the lower buccal vestibule intraorally. Microscopy revealed the sporadic presence of hyperplastic stratified squamous epithelium of variable thickness showing multiple areas of separation from underlying moderately collagenous capsule. Few areas show basilar budding as well as focal basal palisading within the epithelium. One separate tissue shows a dense presence of histiocytes, multinucleated giant cells, and endothelial cells proliferating into the underlying stroma. High power reveals histiocytes displaying nuclear hyperchromatism and pleomorphism in a few areas. These cells were immunopositive for CD68 and immunonegative for p40, Pan-CK, and p53. The ki67 proliferation index was found to be low (Figure 4).
|
|
|
|
|
a) |
b) |
c) |
|
|
|
|
|
d) |
e) |
f) |
|
Figure 4. Case 6–Hybrid lesion of Odontogenic keratocyst with giant cell granuloma displaying parakeratotic lining (a; H&E;10X), highly cellular stroma with histiocytes, multinucleated giant cells (b,c; H&E;20X,40X), CD68 positive histiocytes (d), low Ki67 (e) and negativity to PanCK (f). |
||
Differential diagnosis: As the lesion was highly cellular so differentials of squamous cell carcinoma and histiocytic sarcoma were considered. A low Ki67 index was indicative of benign behavior and CD68 positivity suggested histiocytic cells. The final diagnosis of Odontogenic keratocyst with giant cell granuloma was given.
Giant cell lesions, though commonly encountered in pathologies of the oral cavity, have not been explored systematically with respect to their diagnostic significance. A literature search to date revealed either case reports of single giant cell lesions or case series of one particular type of giant cell lesions. To the best of our knowledge, there is no study describing case series of multiple giant cell lesions together with the emphasis on differential diagnosis and approach for diagnosing these lesions. Individual case reports are of limited assistance to the pathologist challenged by a giant cell lesion. Hence, the need for a systematic algorithm, aimed at a diagnostic approach toward giant cell lesions, cannot be overstated. The frequency of GCLs in our institute was 2.3% whereas Mohajerani et al. reported around 6.2% of GCLs in Iran.[4] This epidemiological difference may be attributed to regional variability in the prevalence of these lesions or the submission of biopsy material to pathologists.
The GCLs are histologically classified into peripheral and central giant cell lesions to further narrow the differentials (Figure 5). Giant cell-rich lesions of bone, also termed central lesions, encompass morphologically diverse tumors of the skeleton. Literature findings of these central lesions reported within jaws are tabulated in Table 3.
Table 3. Differential diagnosis of Central giant cell lesions |
|||||||||
|
Central Giant Cell Lesions |
Age |
Sex |
Site |
Clinical features |
Radiographic |
Histopathology |
Serum Ca |
Serum P |
Serum ALP |
|
Central giant cell granuloma (non-neoplastic lesion) |
<30 years |
F>M |
Exclusively in jaws Anterior mandible crossing midline |
Asymptomatic, seen during routine radiographic examination, Non-aggressive form- Painless expansion of affected bone, Aggressive form- pain, cortical perforation & root resorption. |
Expansile, well demarcated, scalloped border, non-corticated multilocular, less commonly unilocular radiolucency |
Loose fibrillar connective tissue with many interspersed proliferating fibroblasts, hemosiderin laden macrophages and extravasated RBCs, capillaries- small & inconspicuous, multinucleated giant cells are in focal aggregates or patches (zonation phenomenon) or diffusely scattered |
N |
N |
N |
|
Giant cell tumor (osteoclastoma)- benign but locally destructive neoplasm |
3rd – 4th decade |
M>F |
Rare in skull, preferential sites- ends of long bones, the distal femur, proximal tibia, distal radius and proximal humerus, spine and uncommonly flat bones |
Pain, swelling & pathological fracture |
Radiolucent with poorly defined and irregular margins |
Neoplastic stromal component, stromal cellularity is prominent. Mitotic figures may be found. Giant cells are larger with 40-60 nuclei (more than CGCG), homogenous pattern of distribution. May contain inflammatory cells & areas of necrosis but relative absence of hemorrhage & hemosiderin pigment |
N |
N |
N |
|
PHPT |
F>M |
Old age |
Generalized body skeleton disease |
stones, bones, groans and moans |
Osteolytic lesions |
Similar to CGCG |
|
|
N or osteolytic lesions |
|
SHPT |
F>M |
Old age |
Same as PHPT |
Same as PHPT |
Same as PHPT |
Same as PHPT |
|
|
N or in osteolytic lesions |
|
Cherubism – An AD disease SH3BP2 mutation on Chr 4 |
F>M |
2-4 years, regresses after puberty |
Mandible and maxilla
|
Characteristic renaissance cherub faces with rounded jaws, vertical displacement of orbital floor ‘eyes upturned to heaven appearance’, Submandibular and cervical lymphadenopathy-common |
Bilateral symmetrical multilocular radiolucent lesions in the jaw with thick sclerotic borders. Unerupted teeth -‘Floating tooth syndrome’ |
Numerous giant cells in a collagenous stroma, containing abundant fibroblasts. Perivascular eosinophilic cuffing is specific for the lesion |
N |
N |
N (in active growth period there may be physiological increase in ALP) |
|
Noonan like multiple giant cell lesion syndrome-AD |
- |
Congenital anomaly |
- |
Short stature, craniofacial dysmorphisms and congenital heart defects |
Multilocular radiolucency |
Numerous giant cells in a collagenous stroma, containing abundant fibroblasts. Perivascular eosinophilic cuffing is specific for the lesion |
N |
N |
N (in active growth period there may be physiological increase in ALP) |
|
Aneurysmal bone cyst |
M=F |
<20 years |
Nearly every part of skeleton, long bones, vertebral column- common Mandible>maxilla |
Painful firm swelling Two clinicopathologic forms: primary lesion/a secondary lesion (arising in other neoplastic/non-neoplastic osseous conditions) |
Multilocular radiolucency with honeycomb or soap bubble appearance, eccentrically ballooned |
Cavernous or sinusoidal blood filled spaces without endothelial lining. Giant cells (patchy distribution similar to CGCG) along with varying amounts of hemosiderin pigment are present. |
- |
- |
- |
|
Malignant giant cell tumor Very rare sarcoma which arises in juxtaposition to a benign giant cell tumor (primary) or at the site of a previously documented giant cell tumor (secondary). Prognosis of secondary malignant GCT similar to high grade sarcoma worse than primary malignant GCT |
|
|
|
Nonspecific symptoms recurrence of pain and swelling after years of treatment of GCT may suggest possibility of malignant transformation |
Primary presents as lytic process Rarely typical lytic process and sclerotic destructive tumor secondary malignancy- destructive process with poor margination at the site fo previously diagnosed GCT. |
Primary malignancy: area or nodule of highly pleomorphic mononuclear cells in otherwise conventional GCT. Secondary malignant GCT, preexisting GCT may or may not be evident |
- |
- |
- |
These include central giant cell granuloma, giant cell tumor, cherubism, brown’s tumor of hyperparathyroidism, and malignant giant cell tumor. Common to them is CGCG which is a non-neoplastic reparative granuloma where osteoclastic giant cells are distributed within the fibro-cellular stroma.
The present case of CGCG (Case 1 (Figure 1)) is a classic case but no history of trauma is present which is almost always associated with CGCG. The giant cell component may be present in reaction to a recent hemorrhage and a fibroblastic component may represent the older or healing part of the lesion.[7] The exact origin of giant cells in giant cell granulomas remains unclear. The proposed cells of origin for these giant cells include osteoblasts, mononuclear cells from the phagocytic system reacting to hemorrhage, endothelial cells, spindle-shaped mesenchymal cells (reactive population), foreign body cells, and osteoclasts.[8]
The closest mimic of CGCG histopathologically is Brown’s tumor. Additionally, the latter shows multifocal lesions, increased parathormone, hypercalcemia, and hypophosphataemia.[9] Ultrasound, CT scan, or technetium scan techniques can also be used to detect the diseased parathyroid gland.[9, 10] Case 3 in the present study shows multiple osteolytic lesions in the mandible and clivus with histopathology of giant cell granuloma and prominent areas of hemorrhage. An increase in serum PTH levels favored the diagnosis of Brown tumor of HPT. Thus, it is strongly recommended that CGCG should be a diagnosis of exclusion and must be inspected for primary HPT.
Another differential diagnosis of intraosseous giant cell lesions is Cherubism. It is characterized by symmetrical enlargement of jaws limited to the mandible and maxillary bones. It is inherited as an autosomal dominant trait with a mutation in the SH3BP2 gene. SH3BP2 plays a role in regulating the increased osteoblast and osteoclast activities that are seen in normal tooth eruption, and point mutations in the gene could cause pathologic activation of multinucleated osteoclasts, thus causing features of osteolysis and multiple unerupted teeth.[11] Our case (Case 2 (Figure 1)) was a classic case of cherubism presented in a 10-year-old female, with bilateral symmetrical lesions on the mandible, multiple unerupted teeth, and giant cells in histopathology.
Giant cell lesions (GCLs) are further histologically classified into peripheral lesions which are the ones occurring in the gingiva, buccal mucosa, and tongue. The most common lesion occurring in this location is PGCG which is quite distinct with peaks in incidence during the mixed dentitional years and in the age group of 30–40 years. There is also a growing opinion that giant cells in PGCG may simply represent a reactionary component of the lesion and are derived via bloodstream from bone marrow mononuclear cells. They may be present only in response to an as-yet-unknown stimulus from the stroma.[12] The origin from osteoclasts remaining from resorption of deciduous teeth explains its commonest site anterior to permanent molars.[11] Other GCLs that can occur in this location are bacterial, fungal, and foreign-body granulomas. Tuberculosis is the most common chronic bacterial infection, in this part of the world, according to epidemiological studies. The etiologic agent of tuberculosis, M. tuberculosis, is clinically one of the most common microbial causes of granulomas. While caseating granulomas are the classic finding in cases of tuberculosis, they are not always present; non-caseating granulomas may also occur.[13] Our case (Case 3 (Figure 2)) showed non-caseating granulomas. Special stains like ZN stain are used to see bacilli in the sample. Our case revealed negative ZN staining which is concurrent with the observations that acid-fast bacilli could be reliably demonstrated in only 27-60% of cases, owing to the scarcity of bacilli in the tissue.[6]
|
|
|
Figure 5. Diagnostic algorithm for the accurate pathological characterization of giant cell lesions |
The closest mimic of CGCG histopathologically is Brown’s tumor. Additionally, the latter shows multifocal lesions, increased parathormone, hypercalcemia, and hypophosphataemia.[9] Ultrasound, CT scan, or technetium scan techniques can also be used to detect the diseased parathyroid gland.[9, 10] Case 3 in the present study shows multiple osteolytic lesions in the mandible and clivus with histopathology of giant cell granuloma and prominent areas of hemorrhage. An increase in serum PTH levels favored the diagnosis of Brown tumor of HPT. Thus, it is strongly recommended that CGCG should be a diagnosis of exclusion and must be inspected for primary HPT.
Another differential diagnosis of intraosseous giant cell lesions is Cherubism. It is characterized by symmetrical enlargement of jaws limited to the mandible and maxillary bones. It is inherited as an autosomal dominant trait with a mutation in the SH3BP2 gene. SH3BP2 plays a role in regulating the increased osteoblast and osteoclast activities that are seen in normal tooth eruption, and point mutations in the gene could cause pathologic activation of multinucleated osteoclasts, thus causing features of osteolysis and multiple unerupted teeth.[11] Our case (Case 2 (Figure 1)) was a classic case of cherubism presented in a 10-year-old female, with bilateral symmetrical lesions on the mandible, multiple unerupted teeth, and giant cells in histopathology.
Giant cell lesions (GCLs) are further histologically classified into peripheral lesions which are the ones occurring in the gingiva, buccal mucosa, and tongue. The most common lesion occurring in this location is PGCG which is quite distinct with peaks in incidence during the mixed dentitional years and in the age group of 30–40 years. There is also a growing opinion that giant cells in PGCG may simply represent a reactionary component of the lesion and are derived via bloodstream from bone marrow mononuclear cells. They may be present only in response to an as-yet-unknown stimulus from the stroma.[12] The origin from osteoclasts remaining from resorption of deciduous teeth explains its commonest site anterior to permanent molars.[11] Other GCLs that can occur in this location are bacterial, fungal, and foreign-body granulomas. Tuberculosis is the most common chronic bacterial infection, in this part of the world, according to epidemiological studies. The etiologic agent of tuberculosis, M. tuberculosis, is clinically one of the most common microbial causes of granulomas. While caseating granulomas are the classic finding in cases of tuberculosis, they are not always present; non-caseating granulomas may also occur.[13] Our case (Case 3 (Figure 2)) showed non-caseating granulomas. Special stains like ZN stain are used to see bacilli in the sample. Our case revealed negative ZN staining which is concurrent with the observations that acid-fast bacilli could be reliably demonstrated in only 27-60% of cases, owing to the scarcity of bacilli in the tissue.[6]
Hybrid lesions of giant cell lesions have been reported in association with fibro-osseous lesions, Noonan syndrome, neurofibromatosis1, odontogenic keratocyst, and central odontogenic fibroma, etc.[7-13] Our case presented as a rarity of hybrid lesion of odontogenic keratocyst with giant cell granuloma (Case 6 (Figure 4)). This may represent a collision tumor or reactive formation of giant cells in OKC or the possibility of a rare variant.[14]
The additional finding of giant cells without any diagnostic significance was seen in an array of lesions in our study like a radicular cyst, periapical granuloma, fibrous dysplasia, glandular odontogenic cyst, conventional and unicystic ameloblastoma and tumor giant cells in squamous cell carcinoma.[14] MGC reaction in these lesions frequently represents a stromal foreign body reaction to either cholesterol crystals in cystic lesions or keratin from neoplastic epithelial cells or histiocytic in origin.[15]
Conclusion
Histopathology has been traditionally considered as the gold standard for the diagnosis of giant cell lesions. However, the correlation of histopathological findings with clinical, radiological, serological, and ancillary techniques is the key to the proper characterization of GCLs. The classification of these lesions and the algorithmic approach elucidated in this paper, will narrow the differential diagnosis rapidly for the oral pathologist and help in devising a more efficient investigative scheme when these rare lesions are encountered.
None.
None.
None.
Ethics committee approval and informed consent was obtained (IEC-720/04.10.2019, RP-31/2019).
|
||||||||