|
|
|
|
Cisplatin in the Treatment of Lung Cancer: An In Vitro Analysis
S Manish1, K P Ameya2, Dhanraj Ganapathy3, Durairaj Sekar2*
1Saveetha Dental College and Hospital, Saveetha Institute of Medical and Technical Science (SIMATS), Saveetha University, Chennai, India. 2RNA Biology Lab, Saveetha Dental College and Hospital, Saveetha Institute of Medical and Technical Science (SIMATS), Saveetha University, Chennai, India. 3Department of Prosthodontics, Saveetha Dental College and Hospital, Saveetha Institute of Medical and Technical Science (SIMATS), Saveetha University, Chennai, India.
Abstract
Global lung cancer rates are rising, prompting the need for effective treatments. The World Health Organization reports that smoking-related lung cancer is the primary cause of cancer-related deaths worldwide. This study focuses on in vitro analysis of cisplatin for lung cancer treatment, examining the role of STAT3, an essential protein in cell signalling and gene expression. The aim is to gain insights into cisplatin's efficacy, optimal dosage, resistance mechanisms, and potential combination strategies to improve lung cancer treatment protocols and patient outcomes. A549 cells (non-small cell lung cancer) were treated with cisplatin in a 15% fatal bovine serum at 37°C with 5% CO2. Cell viability was assessed using the MTT assay. RNA was isolated using the TRIzol method, and cDNA conversion was performed through thermo-cycling. Gene expression analysis was conducted using qRT-PCR with validated primers and SYBR Premix Ex Taq II. Statistical analysis was carried out using SPSS, and results were presented as mean ± SD. Clinical studies support the efficacy of cisplatin and STAT3 treatment in lung cancer, showing improved survival and reduced metastasis with cisplatin-based chemotherapy. Our experimental study aligns with these findings, highlighting cisplatin's potential in inhibiting lung cancer cell proliferation and migration. As a result of cisplatin treatment, lung cancer cell proliferation and migration were found to be significantly decreased in our study. These results align with other studies that have demonstrated the blocking effects of cisplatin and STAT3 on lung cancer cell proliferation and motility.
Keywords: Lung cancer, Treatment, Cisplatin, Analysis, Cell proliferation
Lung cancer cell line, of which survival for non-small cell lung cancer (NSCLC) is five years of only 10% cell line, is the most prevalent cause of cancer deaths worldwide due to its high prevalence and mortality. Lung cancer takes a heavier toll on lives than breast, prostate, and colorectal cancers combined.[1] In 2020, there were projected to be 2.2 million new instances of lung cancer and 1.8 million deaths from the disease.[2] Small cell lung cancer (SCLC), which accounts for 15% of occurrences, and non-small cell lung cancer (NSCLC), which accounts for around 85% of cases, are the two primary histological forms of lung cancer.[3] 16% of NSCLC patients had an early-stage or localized diagnosis and received surgical resection as treatment.[3, 4] The two primary histological types of lung cancer are small cell lung cancer (SCLC), which accounts for 15% of instances, and non-small cell lung cancer (NSCLC), which accounts for about 85% of occurrences.[5] 16% of NSCLC patients had an early-stage or localized diagnosis and received surgical resection as treatment.[6]
Lung cancer is mainly caused by smoking, with regions with high smoking rates tend to have higher lung cancer rates.[7] Extensive cohort studies have demonstrated the link between smoking cigarettes and lung cancer. According to reports, 90% of lung cancer cases in men and 79% in women are directly related to tobacco usage. An estimated 90% of lung cancer fatalities are thought to be caused by smoking. Compared to non-smokers, lifelong smokers have a twenty to forty times greater risk of developing lung cancer. It has been demonstrated that lung cancer is caused by both different forms of smoking and exposure to ambient cigarette smoke.[8]
A platinum-based chemotherapeutic drug called cisplatin has been essential in the treatment of several solid tumors, including lung cancer.[9] The geometric isomer of cisplatin, trans-DDP, has no impact as a chemotherapy drug. The creation of intrastrand and interstrand crosslinks, which cause structural abnormalities in
DNA, is typically credited with cisplatin's antitumor effect. Cisplatin's DNA adducts are believed to mediate its cytotoxic effects by preventing transcription and DNA replication and, eventually, by triggering apoptosis or programmed cell death. The cis- and trans-DDP adducts are eliminated from DNA via the nucleotide-excision-repair mechanism. Evidence points to a potential involvement for cellular proteins with specific DNA-binding patterns, such as the HMG domain, which bind exclusively to DNA modified by cisplatin but not to trans-DDP DNA adducts.[10] Cisplatin is an anticancer drug that is very effective in treating tumors, yet resistance to this treatment may arise.[11]
STAT3 is an important transcription factor responsible for cell survival, proliferation, and immune responses. STAT3 can be triggered in lung cancer cells by JAK2, IL6, Src, EGFR, or other factors. Protein tyrosine phosphatases, miRNAs, PIAS, SOCS, and PIAS are examples of STAT3 negative regulators.[12] Within the canonical pathway, phosphorylated STAT3 at Tyr705 activates downstream target genes critical for angiogenesis induction, cell proliferation, apoptosis prevention, host immune surveillance evasion, or cancer stem cell self-renewal. Lung cancer cells may also use STAT3 for possible non-canonical purposes.[13, 14]
The National Centre for Cell Science (NCCS), Pune, India, provided the A549 Non-small cell lung cancer cell line, cultivated per the guidelines. It was then nourished with 15% fetal bovine serum (FBS) and maintained at 37 C in a humidified incubator with 5% CO2.
MTT assay was used to explore the effect of cisplatin and combined cisplatin on lung cancer cells on A549 cell viability. In short, A549 cells were seeded in a 96-well round bottom plate (1 x 104 cells per well). At the 12th hour, the cells were incubated at 37°C for four more hours while being exposed to continuous induction from 2.5 up to 80 µm in an orderly fashion (i.e., 2.5 This controlled for the presence or absence of breast cancer cells, using control medium. Cells were allowed to culture for another 48 hours. In this step, MTT reagent was added in all wells, and the mixture was allowed to incubate again for four hours at a temperature of 37°C. Post-incubation and supernatant removal, 150 µl of DMSO was added to dissolve the dye absorbance, read at 490 nm in a microplate reader. This threshold is referred to as IC50, defined as the drug level that induces 50% apoptosis when compared to the negative control.
This experiment had an IC50 of 20 μm. The experiment was done three times, with six parallel samples each.
Total RNA was extracted from malignant and normal samples using the Trizol reagent (Invitrogen, Carlsbad, USA) according to the manufacturer's instructions. The purity and concentration of extracted RNA were evaluated through Nano drop 2000 Lite spectrophotometry (Thermo Fisher Scientific, Waltham, MA). The RNA was kept in refrigeration for more studies at -20°C.
Incubation was done as soon as possible, immediately after cooling of the 10 liters of M-MLV reverse transcriptase reaction mixture. Thereafter, the reaction mixture is thermo-cycled at 30°C for 10 minutes, followed by 42°C for 30 minutes, 95°C for 5 minutes, and then incubated at four °C for the final Quantification of the cDNA by Nano drop lite and storage at -20ºC before analysis comes later. The expression study on the gene TGF was done using SYBR Green (Takara, Japan), and GAPDH was used as a housekeeping control. TGF- primer sequence (forward and reverse) and GAPDH primer sequence (forward and reverse). The following thermos cycling settings were used to amplify the samples in duplicate: 30s at 95°C denaturation with subsequent 40 cycles of 5s at 95°C and 30s at 60°C. Lastly, TGF- expression was quantified using the relative CT (2- Cq) approach.
The TRIZOL reagent was utilized for total RNA extraction. A single-stranded cDNA synthesis was carried out in the presence of 2 ug of total RNA, oligo dT primer, and SII RT. qRT-PCR was carried out on an iCycler with validated primers followed by SYBR Premix Ex Taq II. Transcript levels of specific genes of interest were measured using a cycle-number threshold. During the same incubations, the transcripts were normalized using the housekeeping gene GAPDH as a reference.
This information was represented as mean ± SD. An automated t-test program for comparing TGF levels between cancerous and adjacent normal tissues in the student was utilized. It was found that P =0.05 is considered significant statistically.
The A549 cell line, with its distinctive squamous morphology, provides a relevant model for investigating the intricate processes of electrolyte and water diffusion within the alveoli, reflecting in vivo conditions (Figure 1). Notably adherent to the culture flask, these cells form a monolayer during in vitro cultivation, mirroring the natural growth patterns observed in vivo.
|
|
|
Figure 1. represents A549 lung cancer cells, which are squamous in nature and are responsible for facilitating the diffusion of electrolytes and water throughout the alveoli. These cells adhere to the culture flask and grow as a monolayer when cultured in vitro. |
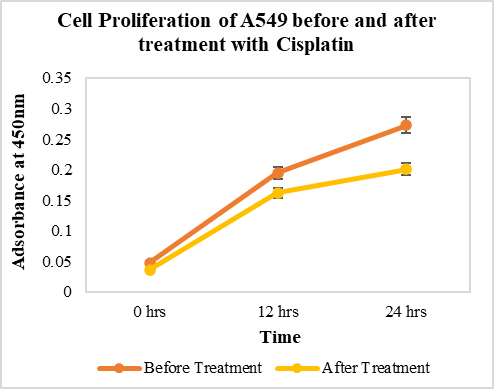
Examining the impact of cisplatin on A549 cells reveals a significant reduction in proliferative rates post-treatment (Figure 2), indicative of a profound modulation in cellular dynamics, suggesting the potential efficacy of cisplatin in impeding uncontrolled growth characteristic of cancer cells within this cell line.
|
|
|
Figure 2. illustrates cells' growth rates before and after treatment with cisplatin. As the graph depicts, the proliferating rate of A549 cells has considerably decreased on account of cisplatin. |
Shifting the focus to the molecular level, the STAT3 gene expression analysis underscores the nuanced cellular response to cisplatin treatment. A discernible decrease in STAT3 gene expression post-treatment, compared to baseline levels in normal lung cancer cells, highlights the intricate regulatory mechanisms influenced by cisplatin within the A549 cell line (Figure 3). This finding emphasizes the significance of STAT3 in lung cancer progression, suggesting its potential modulation by cisplatin as a promising avenue for therapeutic intervention.
|
|
|
Figure 3. shows the expressions of the STAT3 gene before and after treatment of A549 cells with cisplatin. This graph shows that the expression of STAT3 was significantly reduced after the treatment with cisplatin when compared to normal lung cancer cells. |
In this in vitro study, we aimed to assess the synergism between cisplatin, a joint chemotherapy agent, and a STAT3 inhibitor for treating lung cancer in A549 cells.[15] Metastasis-related processes, such as EMT, enhanced cell invasion, migration, and MSC recruitment involving STAT3, were investigated. The study revealed a notable and statistically significant decrease in A549 cell division post-cisplatin treatment, underscoring cisplatin's capacity to induce the destruction of cancer cells.[13, 14, 16]
Furthermore, the gene expression analysis demonstrated a significant reduction in STAT3 concentration after treating the A549 cell line with cisplatin, which is consistent with similar research findings. Combining cisplatin with other chemotherapeutic agents or targeted therapies is explored to enhance overall treatment effectiveness, recognizing the complexity of cisplatin resistance development over time. Ongoing research aims to understand resistance mechanisms, identify predictive biomarkers, and optimize personalized treatment approaches.[17] The intricate interplay between cisplatin and STAT3 suggests a potential avenue for developing targeted therapies, paving the way for more personalized and effective treatment strategies in specific subsets of lung cancer patients.[18, 19]
This study showed the clinical relevance of cisplatin treatment in lung cancer patients and reported improved overall survival and reduced metastasis in patients who received cisplatin-based chemotherapy. This highlights the potential therapeutic benefit of cisplatin in inhibiting lung cancer cell proliferation and migration, as observed in our experimental study. The in vitro analysis of cisplatin in lung cancer treatment provides a foundation for further research and opens up several avenues for future investigations. Some potential areas of future scope for this research include In vivo validation, Clinical trials, Mechanistic studies, Overcoming resistance, Personalized medicine, and Novel drug formulations.
None.
None.
None.
None.
|
||||||||