|
|
|
|
Acute Lymphoblastic Leukemia in Adult Patients: Single Egyptian Center, Six Years Clinical Practice Review
Wedad Hashem1*, Mohsen Mokhtar1, Aisha Abdel Rahman1, Ahmed Rashad1
1Department of Clinical Oncology, Kasr Al Aini School of Medicine; Cairo University, Cairoh, Egypt.
Abstract
Although ALL is a very rare malignancy in adultsit is considered a devastating disease with long-term survival approaching around 30-40%. Proper understanding of the disease biology is the key in ALL management of patients, allowing individualized therapy protocols, as no case is typically like the other, and paving the way to targeted therapy and novel drugs. This is a retrospective study that was performed on 42 patients with newly diagnosed with ALL between January 2015 and December 2020 and were treated with different protocols (all have the same backbone but with different intensity and scheduling) in Kasr Al-Ainy Centre of Clinical Oncology and Nuclear Medicine (NEMROCK). A total of 35 patients diagnosed with ALL were eligible for inclusion in our final analysis. Overall Survival (OS) was 14.4 (95% CI 11.5-17.3) months. It was significantly affected by achieving CR after 1st induction or not, with the median OS for those who achieved CR was 17.9 versus 5.3 months for those who were refractory with a p-value of 0.02. Initial TLC in patients with B-cell ALL significantly affected the OS with longer OS in those who presented with TLC <30,000, with a p-value of 0.03. Disease-free survival (DFS) was 13.3 months; it was significantly affected by achieving CR after 1st induction, with p-values of 0.005. Personalized therapy with risk stratification before treatment initiation and during treatment is an important approach, especially MRD testing, which is a standard of care now in managing all.
Keywords: Adult leukemias, Acute lymphoblastic leukemia, Clinical practice, Therapy protocols
Acute Lymphoblastic Leukemia (ALL) is a malignant clonal proliferation of lymphoid precursors, where normal hematopoietic cells of the marrow are replaced by lymphoid cells, which were blocked at an early stage of differentiation, Thus reducing the number of normal marrow elements. This malignant transformation may originate in the lymphoid cells of different lineages, resulting in B-cell, T-cell leukemia, or mixed-lineage leukemia.[1]
ALL is a highly heterogeneous disease, as it's characterized by genetic alterations blocking cell differentiation and promoting the proliferation of lymphoid precursor cells. Thus, it has many entities affecting risk stratification, prognosis, as well as management strategy plans.[2]
Although ALL is considered one of the most common pediatric malignancies, presenting in 80% of pediatric leukemias, yet the case is different regarding adults ALL; it's a rare disease and only presents in 20% of adult leukemias.[3] With intensified chemotherapy protocols, the survival rates in pediatric ALL approach up to 90%; such a story of success verifies an understanding of the disease biology and treatment strategies originating from clinical studies of children.[1]
Copying the same treatment strategy plans from pediatric protocols had shown an increase in the Complete Remission Rate (CR), yet the long-term disease survival rate (DSF) is still inferior, 30-40% Vs. 80% in adults Vs. Children respectively. [4]
Advances in ALL diagnosis based on biological leukemic cell classification using recent wide genome profiling led to better risk stratification, thus using risk-adapted treatment plans with refinement multi-agent chemotherapies as well as targeted therapy.[3] The landscape of ALL management has changed dramatically after the emergence of measurable/minimal residual disease (MRD) testing, which has become the most important prognostic factor.[1, 5]
Proper understanding of the disease biology is the key in ALL management of patients, allowing individualized therapy protocols, as no case is typically like the other, and paving the way to targeted therapy and novel drugs.[6]
The embodiment of targeted therapy agents has markedly improved the survival rates of adult ALL patients. Using recent treatment protocols raised the long-term survival rates to around 80% in Burkitt's lymphoma cases, 50% in B-cell acute lymphoblastic leukemia (B-ALL) patients, and 50-60% in Philadelphia chromosome-positive ALL patients & T-cell ALL (T-ALL) patients.[3] Using intensive pediatric-inspired regimens in adult ALL (AYAs group specifically) has raised CR rated to 85-90% and long-term EFS & OS to 60-70%.[5, 7]
Initial CNS involvement at the time of diagnosis is not very common, accounting for 5-10% of cases. However, around 50-75% of the patients will develop CNS relapse within the first year if CNS prophylaxis is omitted, and this number drops to 5-10% in case CNS prophylaxis is received.[7, 8]
The aim of our study was to identify overall survival, progression-free survival, and pattern of relapse in ALL patients treated at Kasr Al-Ainy Centre of Clinical Oncology and Nuclear Medicine (NEMROCK) from January 2015 till December 2020.
This is a retrospective study that was performed on 42 patients with newly diagnosed with ALL between January 2015 and December 2020 and were treated with different protocols (all have the same backbone but with different intensity and scheduling) in Kasr Al-Ainy Centre of Clinical Oncology and Nuclear Medicine (NEMROCK). The diagnosis of ALL was based on the presence of blasts in peripheral blood smears or > 20% of lymphoblasts in bone marrow examination and was confirmed by immunophenotyping and cytogenetic and /or molecular studies.
Most of the patients were treated with the same regimen, the "Spanish protocol" (inspired by PETHMA ALL-96 protocol) (Table 1); other protocols used were APO, Hyper-CVAD, MRC UK ALL, and REZ-BFM. Imatinib or dasatinib was added to the protocol in the case of Philadelphia positive. All patients received supportive treatment through the follow-up period.
Table 1. Spanish protocol |
||
|
Induction phase |
||
|
Vincristine 2mg. IV |
On days 1,8,15,22 |
|
|
Doxorubicin 25mg/m2 |
On days 1,8,15,22 |
|
|
Asparaginase 10,000 IU/m2 |
On days 10-12, 17-19, 24-26 |
|
|
Cyclophosphamide 1000mg/m2 |
On day 36 |
|
|
Prednisone 60mg/m2 |
From D1 to 28 |
|
|
CNS prophylaxis: D1, D29 IT Methotrexate 15mg + Hydrocortisone 20mg + ARA-C 30mg. |
||
|
Consolidation I |
||
|
6-Mercaptopurin 50mg/m2 po |
From D1-D7 |
|
|
Methotrexate 3gm/m2 with leucovorin rescue |
On days 1,28,56 |
|
|
VP 16 150mg/m2 IV |
On days 14,42 |
|
|
ARA-C 500mg/m2 IV |
On days 14-15, 42-43 |
|
|
CNS prophylaxis: D1, D29 IT Methotrexate 15mg + Hydrocortisone 20mg + ARA-C 30mg. |
||
|
Drugs |
Consolidation II |
|
|
Vincristine 2mg IV |
On days 1,8,15 |
|
|
Doxorubicin 25mg/m2 |
On days 1-2, 8-9, 15 |
|
|
Asparaginase 10,000 IU/m2 |
On days 1-3, 15-17 |
|
|
Cyclophosphamide 600mg/m2 |
On days 1, 15 |
|
|
Dexamethasone 10mg/m2 then 5mg/m2 |
On days d1-14, then d15-21 |
|
|
CNS prophylaxis: D1, D29 IT Methotrexate 15mg + Hydrocortisone 20mg + ARA-C 30mg. |
||
|
Drugs |
Maintenance |
|
|
Methotrexate 20mg/m2 |
Weekly from week 1-52 |
|
|
Mercaptopurine 50mg/m2 |
Daily from weeks 1-52 |
|
Data were collected by reviewing the patient's electronic medical records at Kasr Al-Ainy Center of Clinical Oncology. Records with incomplete data (7 patients) were omitted. Every patient has a file with a private code number to ensure the privacy of our patients. Data was stored and accessible to the study investigators only. No third party had access to any identifiable patient data except REC and health authorities. No potential risks are expected for the included patients, as data will be extracted from records with no intervention. Data that were collected included age, sex, history, physical examination, and initial laboratory investigations, including complete blood count (CBC), BM aspiration, immunophenotyping, cytogenetics, BCR-ABL1 testing, and different treatment approaches with the follow-up data.
Patients, while receiving treatment, were followed up on different basis, either on admission or in outpatient clinics. Response assessment was followed up with CBC and BMA according to the regimen timeline, along with routine labs, physical examination, and subjective response. Patients are kept under follow-up through different phases of the treatment: induction, consolidation, and maintenance. Patients with BCR-ABL1 positive were followed up through testing it, while other patients followed up with CBC, BMA, and detailed history for any anticipant relapse.
Treatment response was assessed at several points of time throughout the treatment duration.
Statistical analysis will be conducted using SPSS 22nd edition; numeric variables such as age and BMI will be presented in mean ± Standard deviation and compared using student t-test. Categorical data will be presented in frequency and percentage and compared using the Chi2 test. Survival analysis will be conducted using the Log-rank test and Kaplan Meier curve. Risk factors for relapse and death will be estimated using logistic regression analysis after correction for confounding factors. Any p-value <0.05 will be considered significant.
Results and Discussion
In this retrospective study, a total of 35 patients diagnosed with ALL were eligible for inclusion in our final analysis; they had a mean age of 33.7 ± 10.7 years (range: 21-55 years), 62.9% was below 39 years (AYAs), and 37.1% was above 39 years. In our cohort, 45.7% were females and 54.3% were males. Patients’ characteristics and initial presentation are shown in Tables 2 and 3, respectively.
Table 2. Patients’ characteristics. |
|||
|
|
Median/ count |
SD/ percent |
|
|
Age (years) |
33.7 |
10.7 |
|
|
Age groups |
<39 years |
22 |
62.9% |
|
=> 39 years |
13 |
37.1% |
|
|
Comorbidities |
No |
27 |
77.1% |
|
Yes |
8 |
22.9% |
|
|
Type of comorbidity |
None |
27 |
77.1% |
|
Bronchial asthma |
1 |
2.9% |
|
|
Diabetes |
1 |
2.9% |
|
|
Drug addict |
1 |
2.9% |
|
|
Down syndrome |
1 |
2.9% |
|
|
HCV |
2 |
5.8% |
|
|
Hypertension |
1 |
2.9% |
|
|
Rheumatoid arthritis |
1 |
2.9% |
|
|
Virology |
No |
32 |
91.4% |
|
Yes |
3 |
8.8% |
|
|
Type |
Free |
32 |
91.4% |
|
CMV |
1 |
2.9% |
|
|
HCV |
2 |
5.7% |
|
Table 3. Initial presentations among the included patients. |
|||
|
|
Median/ count |
SD/ percent |
|
|
Constitutional |
No |
8 |
22.9% |
|
Yes |
27 |
77.1% |
|
|
initial Symptoms |
No associated symptoms |
21 |
60.0% |
|
Dyspnea |
2 |
5.7% |
|
|
Headache |
1 |
2.9% |
|
|
HSM |
2 |
5.7% |
|
|
Hypertension |
1 |
2.9% |
|
|
Jaundice |
2 |
5.7% |
|
|
Lymphadenopathy |
4 |
11.4% |
|
|
Multi-organ failure |
1 |
2.9% |
|
|
Skin lesions |
1 |
2.9% |
|
|
No |
28 |
80.0% |
|
|
Yes |
7 |
20.0% |
|
|
Site |
No |
28 |
80.0% |
|
Brain |
1 |
2.9% |
|
|
GIT |
1 |
2.9% |
|
|
Kidney |
1 |
2.9% |
|
|
Liver |
1 |
2.9% |
|
|
Lung |
1 |
2.9% |
|
|
Mediastinal |
1 |
2.9% |
|
|
Skin lesions |
1 |
2.9% |
|
|
CNS involvement |
No |
33 |
94.3% |
|
Yes |
2 |
5.7% |
|
The median total leukocyte count (TLC) was 22 x103/cc, ranging from 2.8 to 355 x103/cc, Initial TLC was available in 21 patients with B-cell out of 26 and 10 out of 21 initial count was >30,000, and 5 out of 9 patients with T-Cell initial TLC was available with only 1 patient had TLC >100,000. Bone marrow aspirate and biopsy showed median infiltration of bone marrow by blasts 95% (range 30-100%). Twenty-six (74.3%) patients had B cell lineage leukemia, and 9 (25.7%) patients had T cell lineage leukemia. The cytogenetic study revealed 18 patients (65.85%) had Philadelphia chromosome negative, and 8 patients (22.9%) were Philadelphia chromosome-positive; regarding the B-cell ALL cohort, 8 patients (30.7%) were BCR-ABL1 positive, and 18 patients (69.2%) were BCR-ABL1 negative.
The vast majority of cases were managed by induction using Spanish protocol 82.9% (n=29); other protocols used were APO, Hyper-CVAD, MRC UK ALL, and REZ-BFM. Twenty-two (62.9%) patients had treatment interruptions, 8 patients complained of infection, 4 patients had neutropenia, and 3 patients had refractory disease to the induction protocol.
Among the 8 positive BCR-ABL ALL patients, 7 received imatinib, and one received dasatinib. CNS prophylaxis (doublet/triplet intrathecal) was received by all patients.[10]
Those who achieved CR (23 patients) were assigned for consolidation protocol, and those who were refractory (12 patients) were assigned for re-induction. Only 3 patients achieved CR after re-induction, raising the total number of patients achieving CR to 26 (74.2%) out of 35 patients that were included in our study.
Among those patients who achieved CR either after 1st or 2nd induction, 17 out of 26 (65.3%) patients had relapsed [eight (47%) patients with medullary relapse, 7 (41%) patients medullary & extra-medullary, and 2 (11.7%) patients had isolated extra-medullary relapse]; with median DFS about 13 months. Nine patients out of 17 had CNS relapse either isolated or with medullary relapse, and 3 out of the 9 patients had CNS relapse within 1 year of the diagnosis.
Six (23%) patients had maintained the CR; 5 of them were B-cell ALL (3 patients were Philadelphia positive and were on TKIs), and 1 was T-cell ALL. Three patients had lost Follow-up.
Regarding CNS relapse/Involvement among patients, 11 patients (31.4%) developed CNS relapse, either after achieving CR (9 patients) or developing CNS involvement in the course of refractory disease (2 patients).
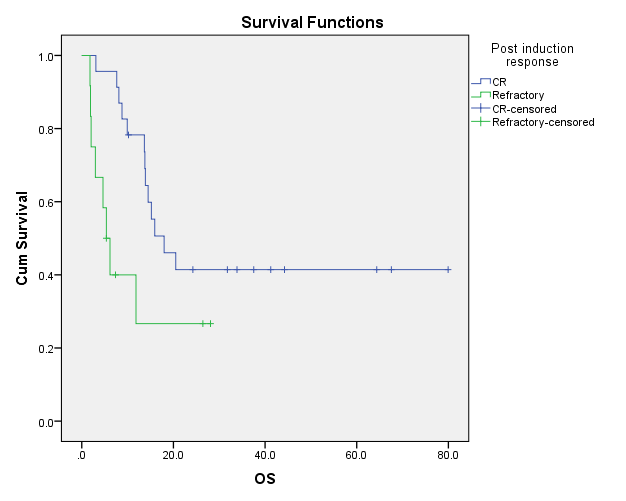
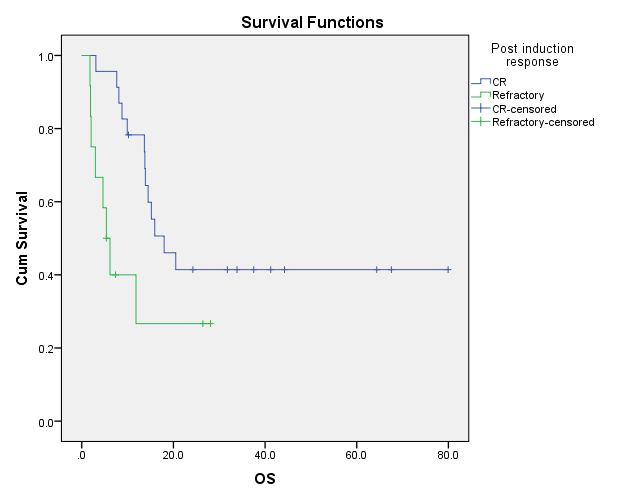
Overall Survival (OS) was 14.4 (95% CI 11.5-17.3) months. It was significantly affected by achieving CR after 1st induction or not, with the median OS for those who achieved CR was 17.9 versus 5.3 months for those who were refractory with a p-value of 0.02 (Figure 1). Among the included patients, 11 patients (31.4%) reached 2 years of OS.
Of clinical importance: Age, subtype, comorbidities, nodal &/or extra-nodal involvement, and interruptions during induction didn’t significantly affect the OS. Initial TLC in B-cell significantly affected the OS. However, initial TLC in T-cell wasn’t statistically significant, affecting the OS. However, the media’ OS with patients presented with TLC > 100,000 Was 8.7 months Vs 11.8 for those presented with TLC <100,000 with a p-value of 0.083.
|
|
|
Figure 1. Kaplan Meier curve showing OS in months according to post-induction response. |
Initial TLC in patients with B-cell ALL significantly affected the OS with longer OS in those who presented with TLC <30,000, with a p-value of 0.03 (Figure 2).
|
|
|
Figure 2. Kaplan Meier curve showing OS in months according to initial TLC in B-cell ALL. |
There is no significant difference in OS according to ALL subtypes with a p-value of 0.63.
Although numerically better, there was no significant difference in OS according to BCR-ABL status. However, patients with BCR-ABL +ve status showed better median OS not reached along the follow-up period Vs 13.6 months for those who were -ve, with a p-value of 0.056.
Disease-free survival (DFS) was 13.3 months; it was significantly affected by achieving CR after 1st induction with longer DFS among patients who achieved CR after induction protocol 21.6 months versus 4.2 months among those who had a refractory disease after induction, with p values 0.005 (Figure 3).
Although initial TLC showed no significant difference in DFS, however, those with B-cell ALL presented with initial TLC >30,000 had lower median DFS with 8.5 months Vs. 29.9 with those who had initial TLC <30,000, with a p-value of 0.070.
Also, initial TLC in T-cell ALL has no significant difference in DFS, but those who presented with TLC >100,000 had lower DFS at 2 months Vs 13.3 months with those who had TLC <100,000, with a p-value of 0.083.
Also, comorbidities, age, subtypes, nodal and extra-nodal involvement, BCR-ABL status, and interruptions during induction showed no significance regarding the DFS.
|
|
|
Figure 3. Kaplan Meier curve showing DFS in months according to response after induction protocol |
Although ALL is a very rare malignancy in adults, representing only around 1% of malignancies and accounts for around 20% of adult leukemias,[9] yet it is considered a devastating disease with long-term survival approaching around 30-40%. (4) The Adolescents and Young Adults group (AYAs) is a specific group of age (between 16 and 39 years) that has gained so much interest in the past two decades in oncology as it’s believed that it has a different biological profile.[7] There was a dilemma about whether it should be treated with pediatric or adult protocols.[11] Several studies have reached the conclusion that pediatric regimens gave superior survival rates in AYAs. A meta-analysis including 11 comparative studies showed lower relapse rates, similar non-relapse mortality, and better DFS than patients who had received adult protocols.[12]
Our study included 35 patients with newly diagnosed ALL; they had a mean age of 33.7 ± 10.7 years (range: 21-55 years), and the majority of patients (62.9%) were < 39 years of age (AYAs). Immunophenotyping revealed that 25.7% of patients were T-cell ALL and 74.3% were B-cell ALL, which conforms with the literature that T-cell incidence is higher in adults, reaching up to 25%.[5] Around 23% of our patients were Ph +ve, which also matched the literature that BCR-ABL1 expression increases with age approaching 15-30% of adult B- cell ALL patients and up to 50% by the age of ≥ 50 years.[8]
The majority of patients in our cohort were in the AYAs group. Also, 11 patients out of 26 with data about the initial TLC showed high-risk TLC, and 8 out of 26 patients were BCR-ABL1 positive. Our management mainly depended on PETHMA protocol ALL-96 which was a trial conducted on standard risk patients (SR ALL was defined in adolescents (age 15 to 18 years) and young adults (age 19 to 30 years) fulfilling all the following criteria: WBC count at or lower than 30x109/L, and absence of t(9;22), t(1;19), t(4;11) or any other 11q23 rearrangements).[13]
Our results were inferior to the results seen in the study that used the same protocol but were nearly comparable to historical results of ALL management among adults when using adult-based regimens that had lower cumulative doses of L-asparaginase steroids.[6] With a complete remission rate (CR) of 65.7% after 1st induction and the total after 2nd induction reached 74.2% (Vs. 98% in PETHMA ALL-96), among those patients, 65.3% of patients had relapsed disease. Median OS was 14.4 months (Vs. 4.2 years in PETHMA ALL-96), and median DFS was 13.3 months (Vs. 6 years DFS was 61% in PETHMA ALL-96). In two years, DFS was 42.8% and 25.7%, respectively. One, two years OS was 60% and 31.4%, respectively. The results discrepancy between our study and the study that used the same protocol could be explained by different risk stratification used in both groups.[13] Another limitation in our study and the PETHMA study was the lack of MRD testing, which is the main prognostic tool now in ALL management, as it redefines the risk groups and assigns patients with high-risk scores to HSCT. This was concluded in (LALA-94 PETHMA ALL 93 trials) which were 2 studies using different treatment regimens with a based protocol used in LALA 94 and Pediatric regimen for the HR group used in PETHMA ALL 93, and HSCT followed as consolidation, showing better outcomes among those who underwent HSCT against those who had not done and had high-risk features, and superior outcomes when HSCT evaded in good responders based on their MRD status.[13] In our cohort, out of 35 patients, only 4 patients had matched siblings; only 1 had HSCT, while the other 3 patients relapsed while arranging for the transplantation.
In our study, it was shown that initial TLC in B-cell lineage significantly affected the OS; although there was no statistically significant difference in T-cell lineage, but it was numerically better results with lower initial TLC; this could be explained by the small sample size. This spotlighted the initial TLC as an important prognostic factor, which mandates categorizing patients with high initial TLC above the cut-off value as high-risk category and assigning them to receive HR intensified regimens.[14, 15]
Although survival outcomes in our study are nearly comparable to the historical results of adult ALL, yet, it are inferior when compared to results from studies that used the same regimens; this is mainly due to the different risk groups between our cohort and the studies' cohort. It signifies the importance of optimizing new strategies to improve the outcome. Personalized therapy with risk stratification before treatment initiation and during treatment is an important approach, especially the MRD testing, which is a standard of care now in managing ALL; also, using intensified chemotherapy regimens with good supportive treatment can improve outcomes with respect to age and risk stratification.
None.
None.
None.
None.
|
||||||||